| Feature | Acute Rheumatic Carditis | Chronic Rheumatic Heart Disease |
|---|---|---|
| Valve leaflets | Edema, inflammation, verrucous vegetations | Fibrosis, calcification, commissural fusion |
| Myocardial lesions | Aschoff bodies (pathognomonic but transient) | Absent; replaced by fibrosis |
| Endocardium | Verrucous vegetations along closure line | Thickened, retracted, stenotic/regurgitant |
| Chronicity | Active, reversible if untreated | Permanent structural deformity |
| Outcome | May resolve with anti-inflammatory therapy | Progressive, requires valve replacement |
Fibrosis and calcification with commissural fusion is the hallmark of chronic RHD and represents the end-stage remodeling that occurs after repeated acute episodes. This is the single best discriminator because it reflects permanent structural damage that cannot be reversed.
Aschoff bodies (granulomatous lesions with Anitschkow cells and Aschoff giant cells) are pathognomonic for acute rheumatic carditis but are transient—they resolve and are replaced by fibrosis in chronic disease. Therefore, Aschoff bodies are absent in chronic RHD.
Verrucous vegetations (small, sterile deposits along the line of valve closure) occur in acute carditis but regress as the disease becomes chronic. In chronic RHD, the valve becomes thickened, retracted, and deformed—not vegetative.
Do not confuse verrucous vegetations of acute rheumatic carditis with those of infective endocarditis (which are larger, destructive, and septic).
Loading illustration…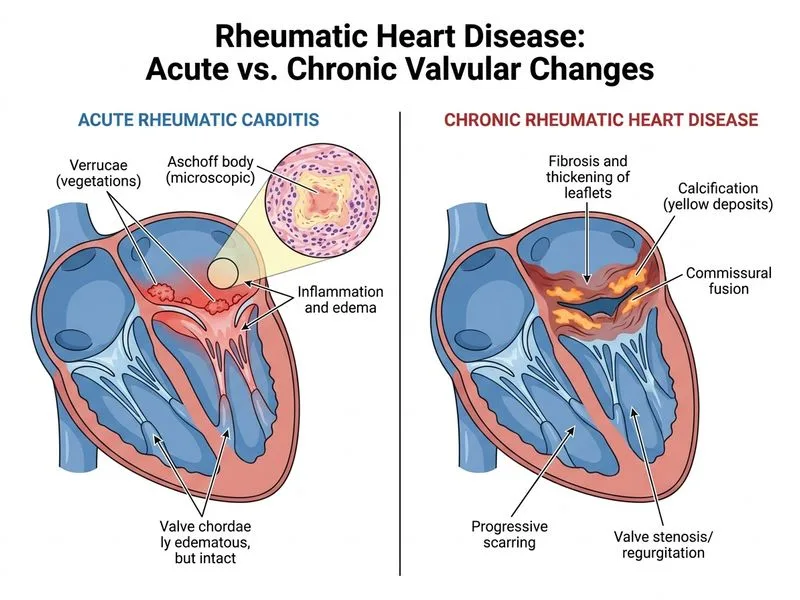
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →