Rotator Cuff and Shoulder Joint MCQ — NEET PG Practice Question | NEETPGAI
Rotator Cuff and Shoulder Joint
medium
bone Anatomy
A 42-year-old female physiotherapist from Mumbai reports chronic left shoulder pain for 8 months with difficulty reaching behind her back to fasten her bra. She has no history of trauma. On examination, the "lift-off test" (Gerber's test) is positive, and she cannot internally rotate the shoulder against resistance. Passive internal rotation is full. What is the most likely rotator cuff muscle involved?
A. Teres major
B. Subscapularis
C. Supraspinatus with secondary subscapularis involvement
D. Infraspinatus with teres minor
Explanation
Subscapularis Tear: Clinical Diagnosis via Lift-Off Test
The Lift-Off Test (Gerber's Test)
Key Point
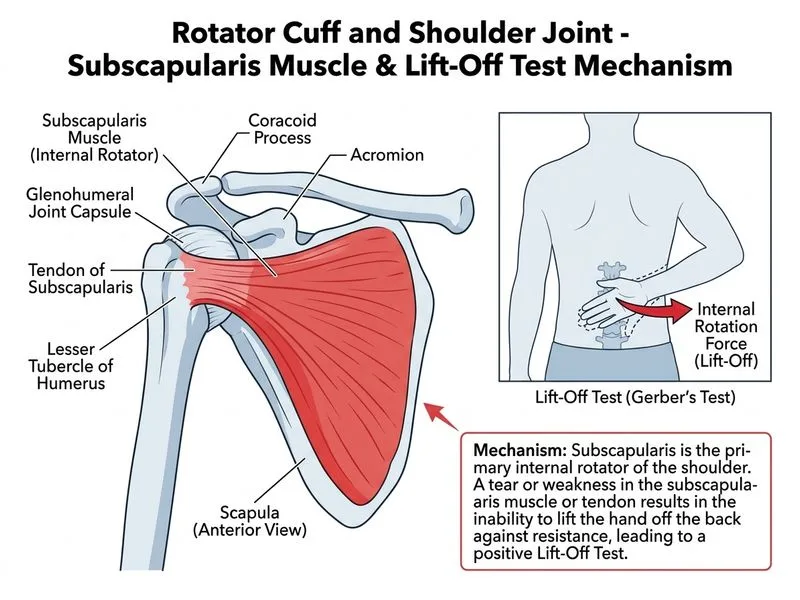
The lift-off test is the gold standard for assessing subscapularis function. The patient places the dorsum of the hand on the lumbar spine and attempts to lift it away from the body (internal rotation against gravity).
Anatomical Basis of the Lift-Off Test
High-YieldNEET PG
The subscapularis is the only muscle capable of internally rotating the shoulder when the arm is behind the back. This position (hand on lumbar spine) isolates subscapularis function:
The arm is adducted and internally rotated
The pectoralis major cannot assist effectively
The latissimus dorsi is stretched
Only the subscapularis can lift the hand away from the spine
Subscapularis Anatomy and Function
Table
Feature
Detail
Origin
Subscapular fossa (anterior scapula)
Insertion
Lesser tubercle of humerus
Innervation
Upper and lower subscapular nerves (C5–C6) from posterior cord
Primary action
Internal rotation (especially with arm adducted)
Secondary action
Adduction and anterior shoulder stability
Clinical test
Lift-off test (Gerber's test)
Why Passive Internal Rotation Is Preserved
Clinical Pearl
Preservation of passive internal rotation in the presence of a positive lift-off test confirms a rotator cuff tear (not capsular restriction). The joint capsule and ligaments are intact, allowing passive motion. The deficit is purely muscular (loss of active force generation).
Differential Diagnosis: Rotator Cuff Tears by Clinical Sign
Table
Muscle
Primary Test
Positive Finding
Loss of Function
Supraspinatus
Drop arm sign
Cannot lower arm from 90° abduction
Abduction 0–15°
Infraspinatus
External rotation lag sign
Lag in external rotation
External rotation
Teres minor
External rotation lag sign
Lag in external rotation
External rotation
Subscapularis
Lift-off test (Gerber's)
Cannot lift hand from lumbar spine
Internal rotation (arm adducted)
Why This Patient's History Fits Subscapularis Tear
1.
Difficulty fastening bra = inability to reach behind back and internally rotate
2.
Positive lift-off test = subscapularis dysfunction confirmed
3.
No trauma = consistent with chronic degenerative tear (common in middle-aged individuals)
4.
Preserved passive ROM = confirms rotator cuff tear, not capsular pathology
Subscapularis Tear: Epidemiology and Pathophysiology
Mnemonic
SITS muscles, but subscapularis is the anterior rotator cuff (the other three are posterior). Subscapularis tears are less common than supraspinatus tears but are associated with:
Chronic overhead activities (her profession as a physiotherapist)
Anterior shoulder instability
Internal impingement
Degenerative changes
Alternative Tests for Subscapularis
Belly-press test (Barth's test): Patient pushes palm against abdomen; positive if elbow flexes (loss of internal rotation strength)
Bear-hug test: Patient hugs chest; inability to maintain position suggests subscapularis weakness
Lift-off test is most specific and sensitive
Why Not Supraspinatus?
Supraspinatus tears present with drop arm sign (inability to lower arm from 90° abduction), not lift-off test positivity. Supraspinatus is responsible for abduction initiation, not internal rotation.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.