## Ruptured AAA with Pancreatic Involvement **Key Point:** Ruptured AAA (rAAA) is a surgical emergency with mortality >50% even with treatment. Management strategy depends on hemodynamic stability and anatomy. **Correct Answer: Permissive Hypotension + EVAR** ### Rationale: - **Hemodynamic instability (SBP 90/60):** Indicates active rupture with ongoing hemorrhage - **Permissive hypotension:** Maintains cerebral and coronary perfusion (target SBP 80–90 mmHg) without aggressive fluid resuscitation, which increases bleeding and mortality - **EVAR vs. open repair:** - **EVAR:** Faster deployment, lower operative mortality (30–35% in rAAA), less blood loss, allows resuscitation time - **Open repair:** Requires aortic cross-clamping, massive blood loss, longer operative time, higher mortality (40–50%) in unstable patients - **Current evidence (IMPROVE trial 2014, EVAR-1):** EVAR is preferred for rAAA when anatomy permits - **Pancreatic involvement:** Secondary to AAA rupture; pancreatic injury is managed after aortic control ### High-Yield: Ruptured AAA + hemodynamic instability → Permissive hypotension + EVAR is modern standard. ### Clinical Pearl: Aggressive fluid resuscitation in rAAA increases bleeding and mortality—"damage control resuscitation" with permissive hypotension is preferred. 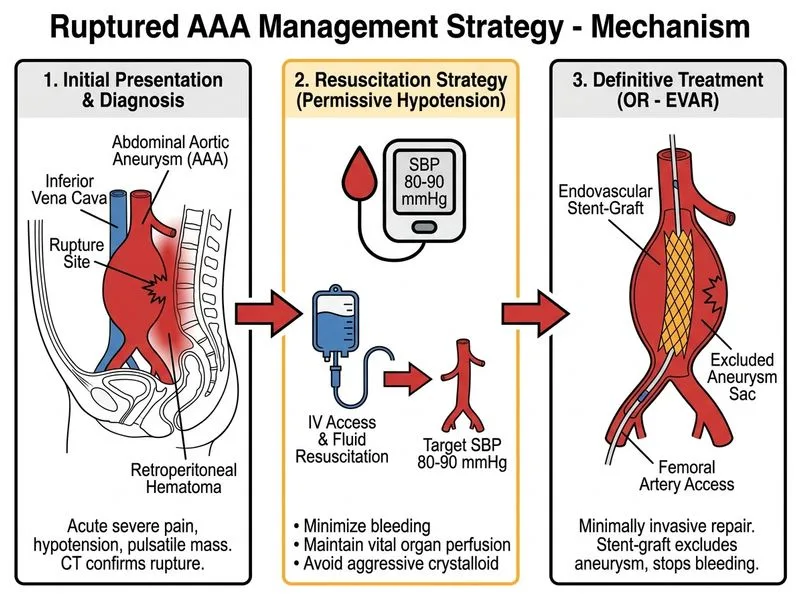
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.