Scabies MCQ — NEET PG Practice Question | NEETPGAI
Scabies
hard
hand Dermatology
A 62-year-old man with advanced dementia and poor hygiene presents with widespread crusted plaques over his entire body, including the face, palms, and soles. He has minimal pruritus despite severe infestation. Microscopy of skin scrapings reveals hundreds of mites. His caregivers report he has not responded to two courses of permethrin applied 1 week apart. What is the most likely diagnosis and the most appropriate next treatment?
A. Bullous pemphigoid; switch to topical corticosteroids
B. Psoriasis; initiate systemic retinoids
C. Crusted scabies; treat with oral ivermectin 200 µg/kg repeated at 1–2 week intervals
D. Atopic dermatitis; prescribe emollients and antihistamines
Explanation
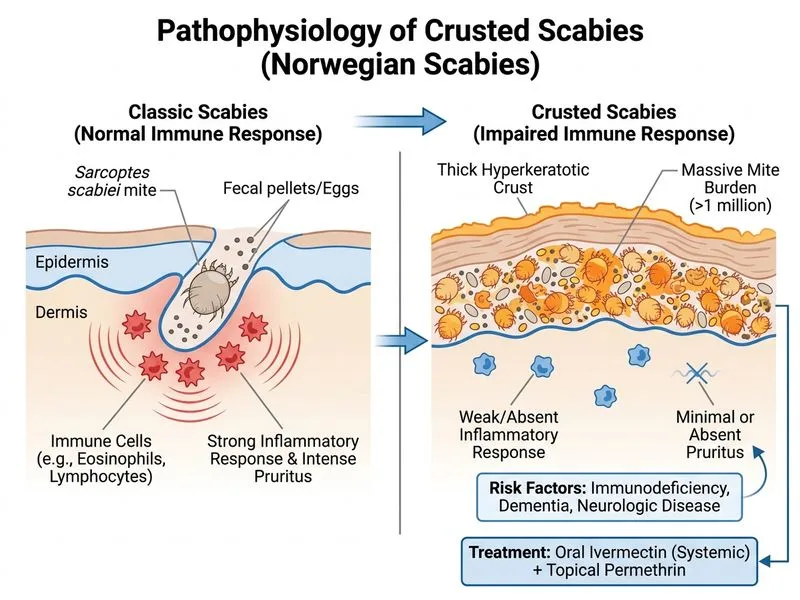
Diagnosis: Crusted (Norwegian) Scabies
Key Point
Crusted scabies is a severe, highly contagious variant characterized by widespread hyperkeratotic crusted plaques, minimal pruritus (paradoxically), and massive mite burden (thousands to millions). It occurs in immunocompromised, elderly, or institutionalized patients.
Clinical Features Distinguishing Crusted Scabies
Table
Feature
Typical Scabies
Crusted Scabies
Mite burden
10–15 mites
Thousands to millions
Pruritus
Intense, nocturnal
Minimal or absent
Distribution
Finger webs, wrists, axillae
Widespread: face, scalp, palms, soles
Morphology
Burrows, papules
Thick hyperkeratotic crusts
Transmission
Skin-to-skin contact
Highly contagious (fomites, respiratory)
Risk groups
General population
Immunocompromised, elderly, institutionalized
Response to topical agents
Excellent
Poor (crusts block penetration)
High-YieldNEET PG
The combination of massive mite burden, crusted plaques, minimal itch, and failure to respond to topical permethrin is pathognomonic for crusted scabies.
Why Topical Agents Fail in Crusted Scabies
1.
Thick crusts act as a barrier, preventing adequate penetration of topical scabicides
2.
Massive mite burden requires systemic therapy for adequate distribution
3.
Immunocompromise (dementia with poor self-care, advanced age) impairs local immune response
Treatment of Crusted Scabies
Key Point
Oral ivermectin is the treatment of choice for crusted scabies.
Ivermectin Dosing
Dose: 200 µg/kg (typically 12 mg for adults)
Schedule: Two doses, 1–2 weeks apart (some sources recommend a third dose at week 3)
Mechanism: Systemic distribution allows penetration through thick crusts and reaches high concentrations in skin
Adjunctive Measures
1.
Keratolytic agents: Salicylic acid 5–10% or urea 10% ointment to soften and remove crusts before ivermectin
2.
Topical scabicides: May be applied after crust removal for enhanced efficacy
3.
Isolation precautions: Crusted scabies is highly contagious; contact isolation recommended in institutional settings
4.
Environmental decontamination: Thorough cleaning of living spaces and frequent laundering of fomites
Clinical Pearl
In this case, the patient's dementia and poor hygiene are risk factors for crusted scabies. The failure of permethrin despite correct application and the massive mite burden on microscopy confirm the diagnosis.
Mnemonic: CRUSTED Scabies Features
C — Crusts (thick, hyperkeratotic) R — Resistant to topical therapy U — Unresponsive to standard permethrin S — Systemic ivermectin needed T — Thousands of mites E — Elderly/Immunocompromised D — Dementia, debilitation
Warning
Do not continue topical permethrin in crusted scabies; it wastes time and allows continued transmission. Switch to oral ivermectin immediately.
Park 26e Ch 8; Fitzpatrick's Dermatology 10e Ch 19
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.