## Clinical Diagnosis: Organophosphate Poisoning with Cholinergic Crisis This patient presents with classic **acute organophosphate toxidrome**: - **Muscarinic signs:** Pinpoint pupils (miosis), bronchospasm, profuse salivation, bradycardia, hypotension - **Nicotinic signs:** Muscle weakness (drowsiness), respiratory depression - **Biochemical:** Severely depressed pseudocholinesterase (18% of normal) - **Blood gas:** Respiratory acidosis with hypoxemia (due to bronchospasm and respiratory depression) ## Pathophysiology Organophosphates irreversibly inhibit acetylcholinesterase, causing accumulation of acetylcholine at synapses and neuromuscular junctions. This leads to: 1. Unopposed cholinergic stimulation (muscarinic + nicotinic receptors) 2. Respiratory failure (bronchospasm + respiratory muscle paralysis) 3. Cardiovascular collapse (bradycardia, hypotension) 4. Death if untreated ## Management Algorithm for Organophosphate Poisoning ```mermaid flowchart TD A[Organophosphate exposure]:::outcome --> B[Decontamination + ABCs]:::action B --> C[Secure airway if needed]:::action C --> D[Atropine: titrate to drying of secretions]:::action D --> E{Muscarinic signs resolved?}:::decision E -->|No| F[Repeat atropine every 5-10 min]:::action E -->|Yes| G[Start pralidoxime infusion]:::action G --> H[Pralidoxime reactivates AChE]:::action H --> I[Continue supportive care]:::action I --> J[Monitor for relapse]:::outcome ``` ## Why Atropine Is First-Line **Key Point:** Atropine is the **immediate life-saving drug** in organophosphate poisoning because it blocks muscarinic receptors, rapidly reversing the life-threatening respiratory and cardiovascular effects. **High-Yield:** Atropine dosing in organophosphate poisoning: - **Initial dose:** 2–5 mg IV bolus - **Repeat:** Every 5–10 minutes until signs of atropinization appear - **Endpoint:** Drying of bronchial secretions, improved bronchial tone, heart rate ≥60/min, systolic BP ≥90 mmHg - **Total dose:** May require 50–100 mg or more in severe cases **Clinical Pearl:** Atropine works rapidly (within seconds) because it blocks muscarinic acetylcholine receptors. It does NOT reverse nicotinic effects (muscle weakness, paralysis) — that is the role of pralidoxime. ## Atropine vs. Pralidoxime: Complementary Roles | Agent | Target | Mechanism | Onset | Effect | |-------|--------|-----------|-------|--------| | **Atropine** | Muscarinic receptors | Competitive antagonist | Seconds | Dries secretions, dilates bronchi, ↑ HR, ↑ BP | | **Pralidoxime (2-PAM)** | Acetylcholinesterase | Reactivates enzyme (nucleophilic attack) | Minutes | Restores enzyme function, reverses nicotinic effects | **Mnemonic:** **SLUDGE** (Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis) — all **muscarinic** effects reversed by **atropine**. ## Sequence of Treatment 1. **Immediate:** Atropine IV bolus (2–5 mg), repeat every 5–10 min until atropinization 2. **Concurrent:** Pralidoxime 1 g IV over 5–30 min (reactivates acetylcholinesterase) 3. **Supportive:** Mechanical ventilation (as done), oxygen, IV fluids 4. **Monitoring:** Repeat pralidoxime every 4–6 hours if needed; watch for relapse **Warning:** Do NOT use neostigmine (an anticholinesterase) — it will worsen the cholinergic crisis by further inhibiting acetylcholinesterase. 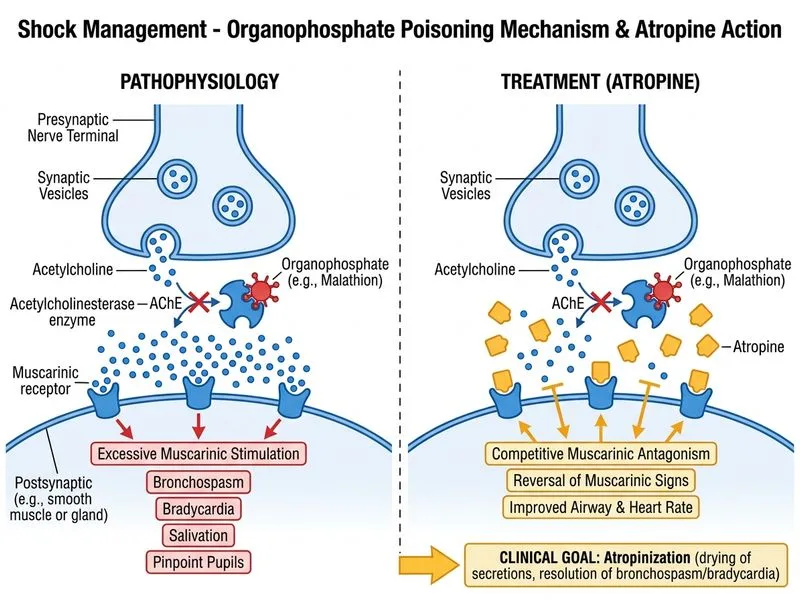
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.