A 24-year-old man of African descent presents to the emergency department with acute onset severe chest pain, dyspnea, and fever (38.5°C). He has a known history of sickle cell disease (HbSS genotype). On examination, he is tachycardic (HR 110/min), tachypneic (RR 28/min), and has decreased air entry in the left lower lobe. Chest X-ray shows a new infiltrate in the left lower lobe. Hemoglobin is 7.2 g/dL (baseline 8.5 g/dL), reticulocyte count is 8%, and LDH is markedly elevated. Blood culture is pending. What is the most likely diagnosis?
A. Acute chest syndrome
B. Pneumonia with sepsis
C. Acute splenic sequestration
D. Pulmonary embolism
Explanation
Diagnosis: Acute Chest Syndrome (ACS)
Clinical Presentation
This patient presents with the classic triad of acute chest syndrome:
1.
Fever (38.5°C)
2.
Chest pain with respiratory symptoms
3.
New pulmonary infiltrate on imaging (CXR)
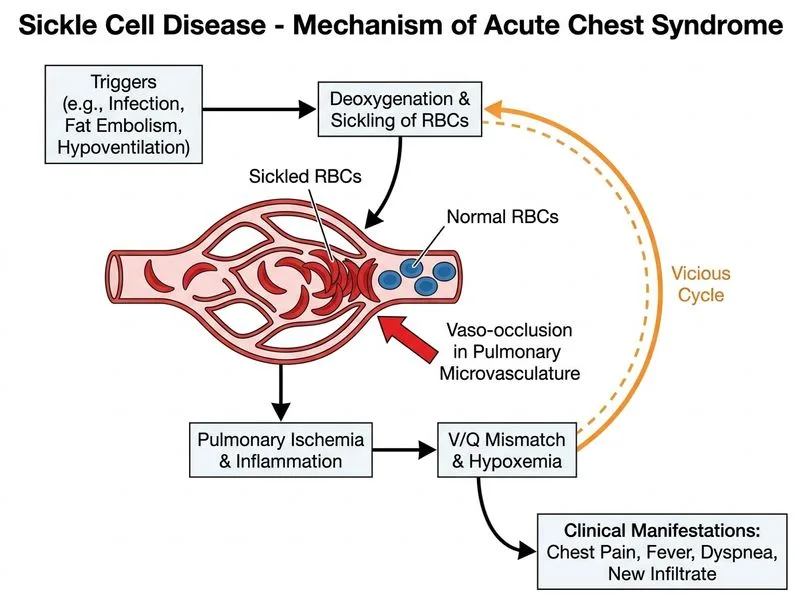
Pathophysiology
Key Point
Acute chest syndrome is a vaso-occlusive crisis affecting the pulmonary vasculature, characterized by sickling of RBCs in lung microvasculature, leading to infarction, inflammation, and secondary infection.
Diagnostic Features
Table
Feature
ACS
Pneumonia
PE
Fever
Common (>50%)
Yes
No
New infiltrate
Yes (consolidation)
Yes
No
Hemoglobin drop
Yes (acute)
No
No
Reticulocyte count
Elevated (>5%)
Normal
Normal
LDH elevation
Marked (hemolysis)
Mild
Mild
Hypoxemia
Yes
Yes
Yes
High-YieldNEET PG
ACS is the second leading cause of death in sickle cell disease (after stroke) and occurs in ~50% of SCD patients at some point.
Pathogenesis
1.
Sickling of RBCs in pulmonary microvasculature
2.
Vaso-occlusion → pulmonary infarction
3.
Release of phosphatidylserine → tissue factor activation
Fat embolism from bone marrow necrosis (if concurrent bone infarction)
Clinical Pearl
Key Point
The acute drop in hemoglobin (7.2 from baseline 8.5) with elevated reticulocytes and LDH indicates acute hemolysis superimposed on vaso-occlusion—this is pathognomonic for ACS, not simple pneumonia.