| Pathogen | Frequency in SCD | Reason | Clinical Feature |
|---|---|---|---|
| **Salmonella (non-typhi)** | Most common | Asplenia + gut translocation | Metaphyseal |
| Staphylococcus aureus | Second most common | Still occurs; asplenia is not absolute | Metaphyseal/diaphyseal |
| Streptococcus pneumoniae | Encapsulated; asplenia | Sepsis/meningitis more than osteomyelitis | Systemic |
| Haemophilus influenzae | Encapsulated; asplenia | Rare post-vaccination | Systemic |
Increased bone marrow cellularity does occur in SCD (extramedullary hematopoiesis), but it does not directly impair blood flow to bone or predispose to infection. It is a consequence of chronic hemolysis, not a cause of osteomyelitis.
Defective neutrophil chemotaxis is not a feature of SCD. Neutrophil counts are often elevated due to chronic hemolysis and inflammation. The problem is not neutrophil function but rather the loss of splenic opsonization.
Chronic hypoxia-induced impaired wound healing is not the mechanism. Bone is well-vascularized in SCD (paradoxically, due to chronic anemia-driven hyperemia), and the issue is immunologic, not vascular.
A — Autoinfarction of spleen (repeated vaso-occlusion) S — Susceptibility to encapsulated organisms (Streptococcus pneumoniae, Haemophilus) P — Predisposition to Salmonella osteomyelitis L — Loss of opsonization and complement-mediated killing E — Encapsulated pathogens + atypical organisms (Mycoplasma, Salmonella) N — Neisseria meningitidis also increased risk I — Impaired IgG and complement responses A — Asplenic crisis (acute hemolytic episode)
Robbins 10e Ch 14; Harrison 21e Ch 104
Loading illustration…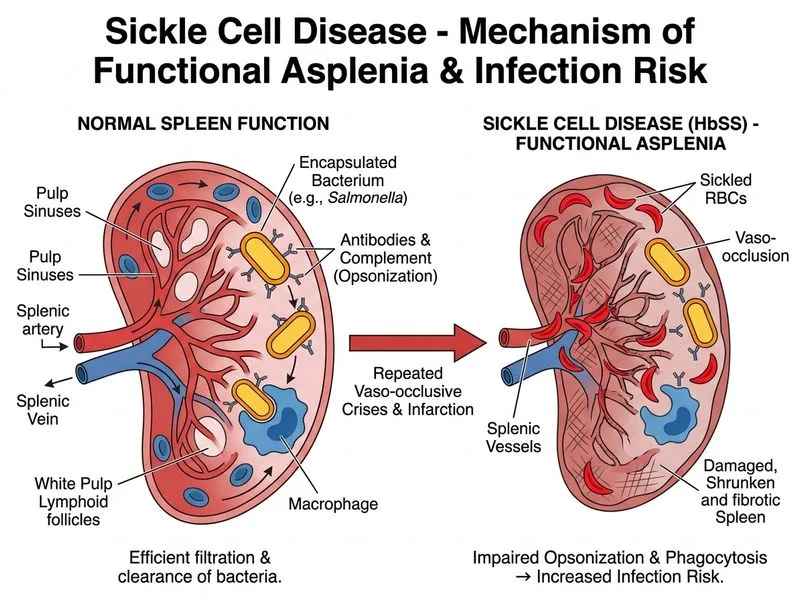
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →