## Splenic Trauma Management Strategy In a **haemodynamically stable patient** with blunt splenic injury, **non-operative management (NOM)** is the standard of care, even for Grade III lacerations. ### Key Principles: - **Haemodynamic stability** is the primary criterion for NOM eligibility - Grade III splenic injuries can be managed conservatively if the patient remains stable - Management includes: - ICU or high-dependency unit admission - Bed rest (initially strict, then progressive mobilization) - Serial clinical examination (abdominal tenderness, peritoneal signs) - Serial haemoglobin checks - Immediate surgical backup availability - Blood products on standby ### Success Rate: - NOM succeeds in >90% of haemodynamically stable patients with blunt splenic injury, regardless of grade - Splenectomy is reserved for haemodynamic instability despite resuscitation or peritoneal signs suggesting ongoing bleeding **Clinical Pearl:** Splenic artery embolization (SAE) is increasingly used as an adjunct in select cases (high-grade injuries with pseudoaneurysm on CT), but observation alone is first-line for uncomplicated Grade III injury in stable patients. 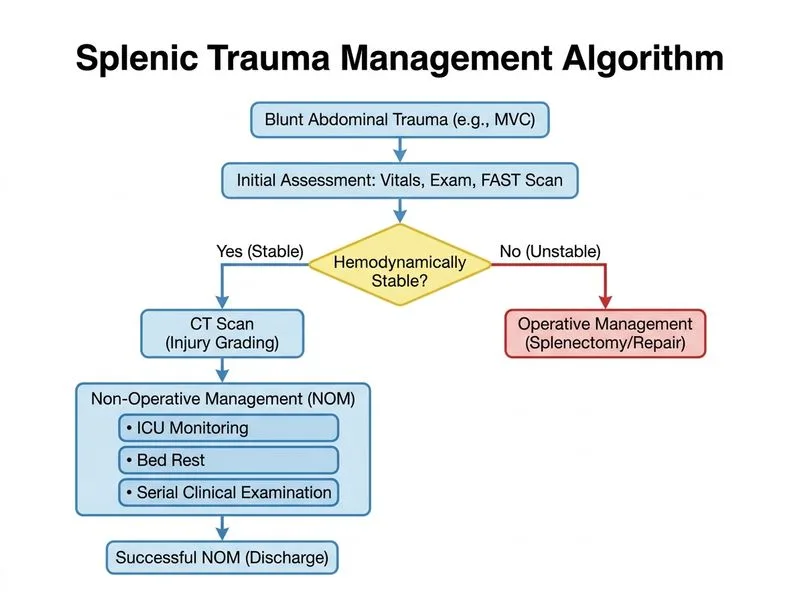
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.