STEMI Diagnosis and Management MCQ — NEET PG Practice Question | NEETPGAI
STEMI Diagnosis and Management
hard
stethoscope Medicine
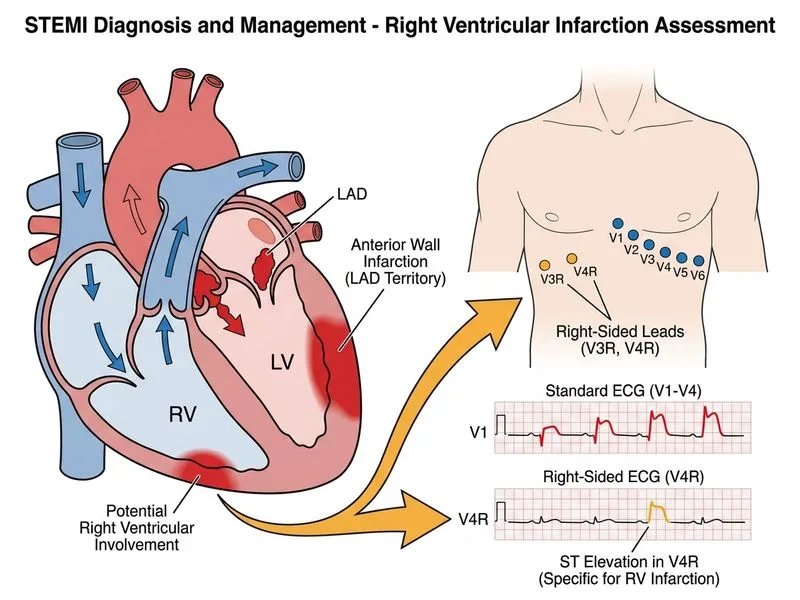
A 52-year-old woman with diabetes and dyslipidemia presents with acute anterior chest pain for 1.5 hours. ECG shows ST elevation in leads V1–V4 with reciprocal ST depression in II, III, and aVF. She is hemodynamically stable. She received aspirin 325 mg and clopidogrel 600 mg in the emergency department. The nearest PCI-capable hospital is 45 minutes away. Which investigation should be performed immediately to assess for right ventricular involvement and guide fluid management?
A. Right-sided ECG (leads V3R–V4R)
B. Pulmonary artery catheterization
C. Cardiac CT angiography
D. Transthoracic echocardiography
Explanation
Right Ventricular Infarction: Diagnosis and Management
Clinical Context
This patient has anterior wall STEMI (ST elevation in V1–V4) with reciprocal changes. The question specifically asks about assessing for right ventricular (RV) involvement.
Key Point
Right ventricular infarction occurs in 30–50% of inferior wall STEMIs but can also occur with anterior STEMIs, particularly when the right coronary artery (RCA) is the culprit vessel. RV involvement has critical implications for hemodynamic management.
Why Right-Sided ECG (V3R–V4R)?
1.
Immediate and non-invasive: Can be performed at the bedside in seconds
2.
Diagnostic accuracy: ST elevation ≥1 mm in V4R has ~90% sensitivity and specificity for RV infarction
Placed on the right side of the chest at the same intercostal levels
V4R is the most sensitive and specific lead for RV infarction
Why Other Investigations Are Inappropriate
Table
Investigation
Limitation
Transthoracic echo
Operator-dependent; takes 10–15 minutes; does NOT guide acute hemodynamic decisions as rapidly as ECG
Cardiac CT angiography
Time-consuming; delays transfer to catheterization laboratory; not indicated for acute STEMI diagnosis
PA catheterization
Invasive; not needed for RV infarction diagnosis; reserved for refractory cardiogenic shock
Clinical Pearl
RV infarction is often overlooked because the standard 12-lead ECG does NOT include right-sided leads. Always obtain right-sided ECG in patients with inferior or anterior STEMI who present with hypotension or bradycardia, or when RV involvement is suspected.
Warning
Do NOT give diuretics to a hypotensive patient with RV infarction — this worsens outcomes by reducing preload. The hemodynamic profile is opposite to left ventricular infarction.
Harrison 21e Ch 297
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.