This is an inferior wall STEMI (ST elevation in II, III, aVF with reciprocal ST depression in I, aVL) presenting within 2 hours of symptom onset. The patient is at a non-PCI-capable primary health centre 120 km from the nearest PCI-capable hospital in rural Maharashtra.
High-Yield Calculation:
Option A (aspirin + clopidogrel + immediate transfer for PCI) would be correct only if the PCI centre could be reached within 120 minutes of FMC. A 120 km rural transfer in India realistically takes ≥2 hours for transport alone, making total FMC-to-balloon time >3 hours — unacceptably beyond the guideline threshold. Delaying reperfusion in favour of PCI in this setting increases mortality.
Troponin results are never awaited before initiating STEMI management. ECG diagnosis is sufficient and time-critical. Waiting for biomarkers is explicitly contraindicated in STEMI guidelines.
Arranging transfer for PCI "within 24 hours" is appropriate only for pharmacoinvasive strategy (post-thrombolysis angiography), not as the primary reperfusion plan. Unfractionated heparin alone without thrombolysis is insufficient reperfusion.
STEMI at non-PCI centre
↓
Can PCI be achieved within 120 min of FMC?
YES → DAPT + immediate transfer
NO → Thrombolysis immediately (door-to-needle <30 min)
↓
Streptokinase 1.5 million units IV over 60 min
+ Aspirin 325 mg + Anticoagulation
↓
Transfer for pharmacoinvasive angiography within 3–24 hoursReference: ACC/AHA STEMI Guidelines 2013 (O'Gara et al.), ESC STEMI Guidelines 2017, CSI Consensus Statement on STEMI Management in India.
Loading illustration…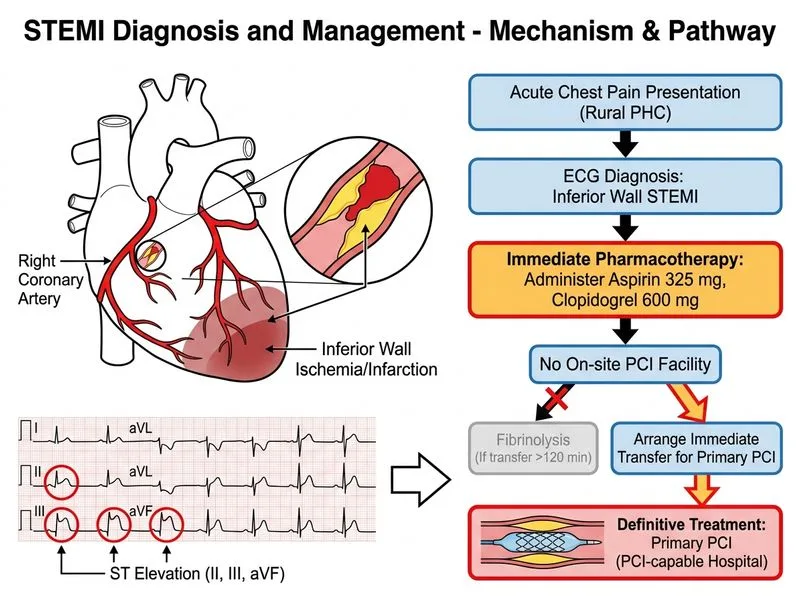
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →