STEMI Diagnosis and Management MCQ — NEET PG Practice Question | NEETPGAI
STEMI Diagnosis and Management
medium
stethoscope Medicine
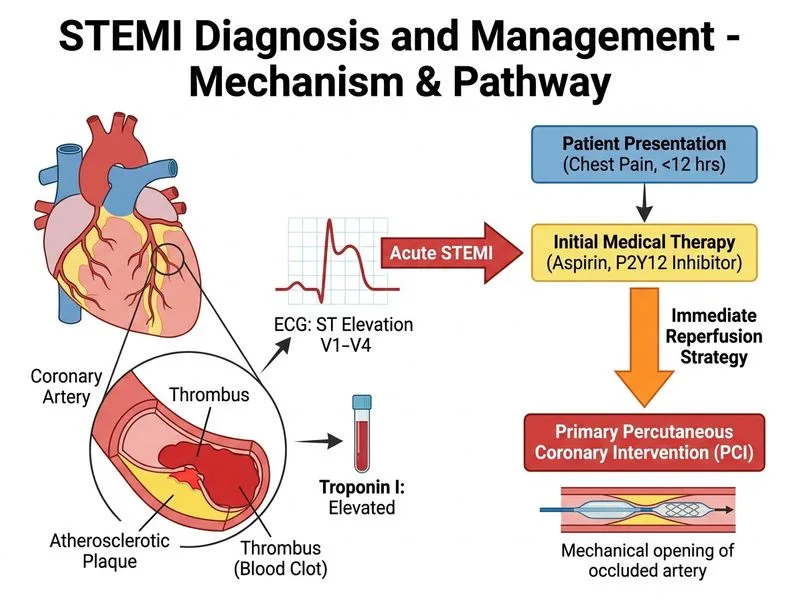
A 62-year-old woman with diabetes and hypertension presents to the emergency department 6 hours after onset of acute anterior chest pain. ECG shows ST elevation in V1–V4 with reciprocal ST depression in II, III, aVF. She has received aspirin 325 mg and clopidogrel 600 mg at a referring centre. Her troponin I is 2.8 ng/mL (normal <0.04). She is haemodynamically stable (BP 128/80, HR 88). The hospital has a functional catheterization laboratory. What is the most appropriate next step?
A. Perform primary percutaneous coronary intervention immediately
B. Administer intravenous thrombolytic therapy (alteplase) and arrange PCI if reperfusion fails
C. Perform stress testing to assess myocardial viability before deciding on revascularization
D. Start high-intensity statin and beta-blocker; perform coronary angiography after 48 hours when troponin plateaus
Explanation
Clinical Scenario Analysis
This is an anterior wall STEMI (ST elevation V1–V4, reciprocal changes in inferior leads) in a PCI-capable hospital presenting 6 hours after symptom onset with established myocardial necrosis (elevated troponin).
Key Decision Points
High-YieldNEET PG
The presence of:
1.
STEMI on ECG (diagnostic, not requiring troponin confirmation)
2.
PCI facility available (in-house catheterization lab)
3.
Symptom onset within 12 hours (still within therapeutic window)
4.
Haemodynamic stability (no cardiogenic shock)
All point to immediate primary PCI as the standard of care.
Time Window for Reperfusion
Key Point
Although the patient is 6 hours from symptom onset, primary PCI remains the gold standard because:
Door-to-balloon time can be achieved within 90 minutes (patient is already in a PCI-capable hospital).
PCI is superior to thrombolysis even in the 6–12 hour window if haemodynamically stable.
Anterior STEMI (LAD territory) carries high mortality; reperfusion is critical.
Clinical Pearl
The 12-hour window is a guideline threshold. PCI is indicated up to 12 hours in stable patients; beyond 12 hours, PCI is reserved for haemodynamic instability or mechanical complications.
Why Not Thrombolysis?
Thrombolysis is not indicated in this scenario because:
1.
Primary PCI is available and superior — thrombolysis is only used when PCI is unavailable or cannot be performed within 120 minutes.
2.
Anterior STEMI has higher mortality — PCI provides better outcomes than thrombolysis in this territory.
3.
Patient is haemodynamically stable — no indication for "rescue" thrombolysis followed by PCI.
Warning
Administering thrombolysis when primary PCI is available is a common exam trap. Thrombolysis is second-line, not first-line, in PCI-capable centres.
Why Not Delayed Angiography?
High-YieldNEET PG
The option to "perform angiography after 48 hours" is incorrect because:
STEMI is a time-critical emergency. Reperfusion must occur within hours, not days.
Delaying angiography results in irreversible myocardial necrosis and poor left ventricular function.
Troponin elevation does not change the urgency — it confirms necrosis has already begun; reperfusion must be expedited, not delayed.
Mnemonic
STEMI = Time is Myocardium — every minute of ischaemia results in irreversible damage.
Management Algorithm
Loading diagram...
Adjunctive Medications
Key Point
The patient has already received DAPT (aspirin + clopidogrel), which is correct. Additional management includes:
Unfractionated heparin (bolus 60–70 U/kg IV) or enoxaparin during PCI.
Glycoprotein IIb/IIIa inhibitor (e.g., abciximab, tirofiban) — considered in high-risk STEMI (anterior wall, large infarct).