## Surgical Management of Bleeding Duodenal Ulcer Refractory to Endoscopy **Antrectomy with Billroth II reconstruction** is the most appropriate surgical procedure for bleeding duodenal ulcer in the modern era. ### Key Point: - **Indication**: Bleeding duodenal ulcer refractory to endoscopic therapy (failed twice) - **Rationale**: Antrectomy removes the gastrin-secreting antrum, reducing acid production - **Reconstruction**: Billroth II (gastrojejunostomy) is preferred over Billroth I in duodenal ulcer disease - **Vagotomy**: **No longer necessary** in the PPI era; PPIs are more effective acid suppressants ### Historical Context: - **Pre-PPI era**: Vagotomy + pyloroplasty or antrectomy + vagotomy were standard - **Post-PPI era**: Vagotomy is rarely indicated; antrectomy alone is sufficient - **Current practice**: Antrectomy ± Billroth II is the procedure of choice ### Why Billroth II? - Billroth II (gastrojejunostomy) is preferred in duodenal ulcer disease - Billroth I (gastroduodenostomy) is preferred in gastric ulcer disease (preserves duodenal passage) - In duodenal ulcer, the duodenum is diseased; Billroth II bypasses it ### Clinical Pearl: **Vagotomy is obsolete** in the PPI era. Modern surgical management of bleeding PUD focuses on antrectomy (removing the acid-secreting antrum) without vagotomy. Perioperative PPI therapy provides additional protection. 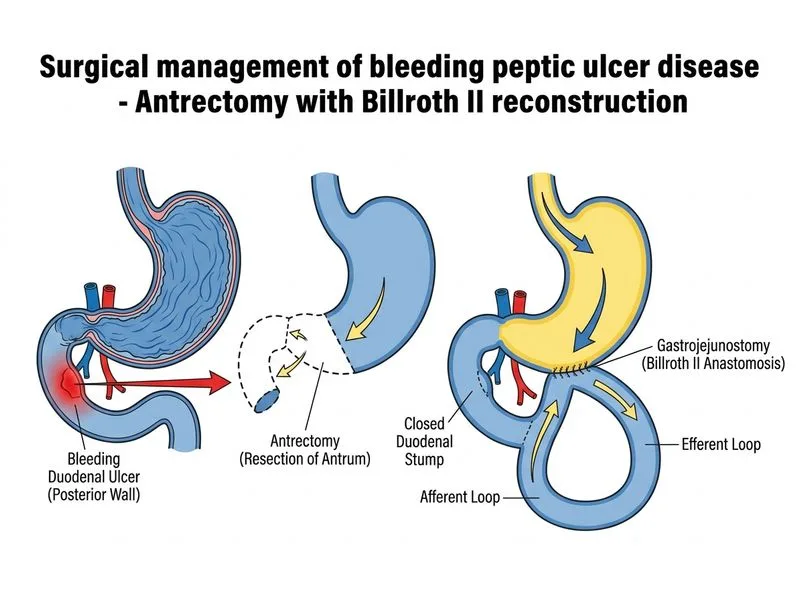
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.