A Bethesda Category III (atypia of undetermined significance / follicular neoplasm) result on FNAC carries a 15–30% risk of malignancy. The nodule is 2.5 cm (>2 cm), which increases suspicion. Repeat FNAC has poor sensitivity and delays diagnosis; observation alone is inappropriate given the size and cytology.
Thyroid lobectomy with intraoperative frozen section is the gold standard for Bethesda III nodules >2 cm. This approach:
Bethesda Category III carries 15–30% malignancy risk. Size >2 cm warrants surgical evaluation rather than repeat cytology or observation alone.
Molecular testing (ThyroSeq, Afirma) can help refine risk in Bethesda III, but in a resource-limited setting or when unavailable, lobectomy with frozen section remains the standard of care in India.
Loading illustration…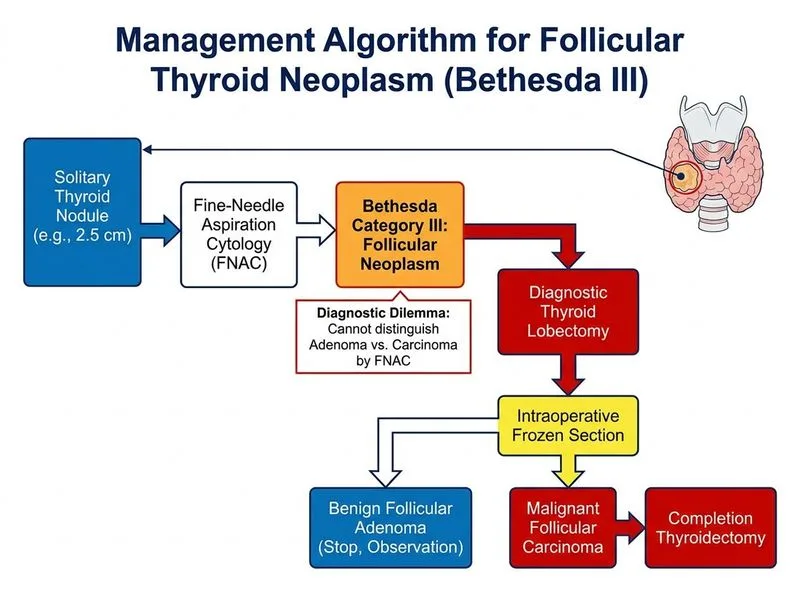
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →