This patient has low-risk PTC (Stage I: <4 cm, no extrathyroidal extension, no lymph node involvement, classical variant). Risk stratification determines the intensity of follow-up and need for radioactive iodine (RAI).
| Feature | Low-Risk | Intermediate-Risk | High-Risk |
|---|---|---|---|
| Tumor size | <4 cm | Any | Any |
| Extrathyroidal extension | Absent | Minimal | Gross |
| Lymph node involvement | None | N1a or N1b | N1b with extranodal extension |
| Distant metastases | Absent | Absent | Present |
| RAI ablation | Not routinely needed | Consider | Recommended |
| TSH target | 0.5–2 mIU/L | 0.1–0.5 mIU/L | <0.1 mIU/L |
Low-risk PTC does NOT routinely require radioactive iodine ablation. TSH suppression to 0.5–2 mIU/L (mild suppression) is appropriate, with surveillance by thyroglobulin and ultrasound.
ATA 2015 Guidelines: RAI ablation is not recommended for low-risk PTC (Stage I, no high-risk features). Aggressive TSH suppression (<0.1 mIU/L) is reserved for high-risk disease and increases cardiovascular and bone morbidity without clear benefit in low-risk patients.
Thyroglobulin is an excellent tumor marker in PTC. Undetectable thyroglobulin on levothyroxine monotherapy with normal ultrasound is reassuring and indicates excellent prognosis in low-risk disease. Serial measurement guides follow-up intensity.
Loading illustration…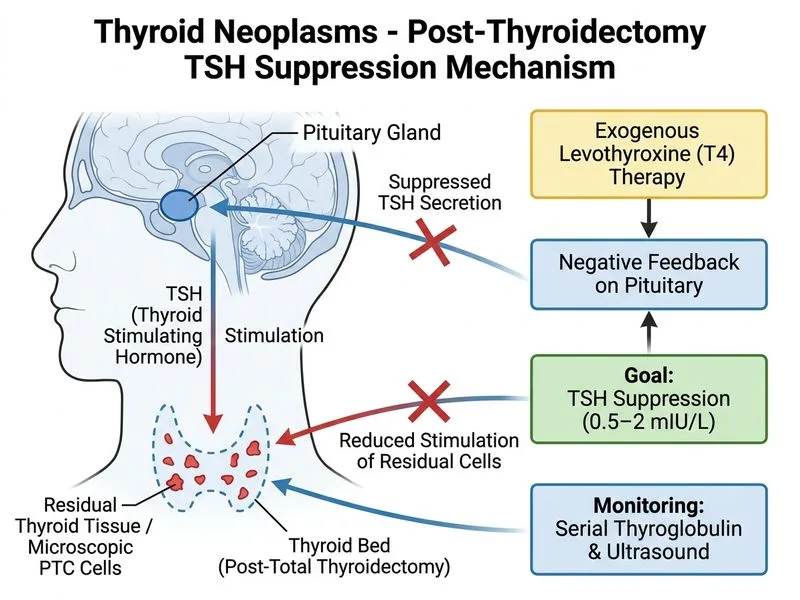
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →