These features are present in PTC regardless of whether the tumor grows in papillary or follicular architecture.
| Feature | PTC | FTC |
|---|---|---|
| Nuclear grooves | Present (diagnostic) | Absent |
| Pseudoinclusions | Present | Absent |
| Chromatin pattern | Pale, fine (Orphan Annie) | Coarse, darker |
| Capsular invasion | Not required for diagnosis | Required for diagnosis |
| Vascular invasion | Not required for diagnosis | Required for diagnosis |
| Follicular architecture | May be present | Always present |
| RAS/BRAF mutations | BRAF V600E common | RAS mutations common |
Capsular and vascular invasion are required for FTC diagnosis but are not present in most PTC cases. However, they do not distinguish PTC from FTC — rather, their presence in a follicular-patterned tumor with normal nuclei defines FTC. They are not a feature of PTC itself.
Robbins 10e Ch 24
Loading illustration…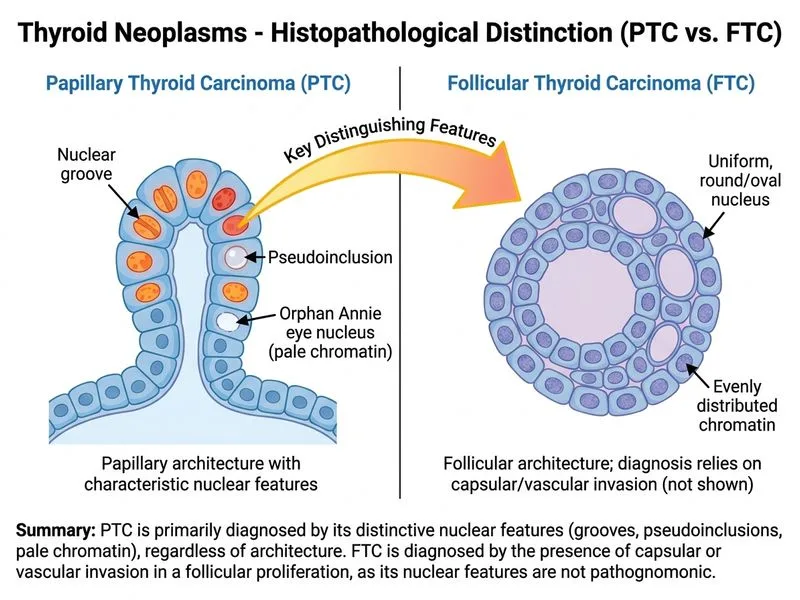
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →