## Clinical Context This patient has a **symptomatic multinodular goiter (MNG)** with: - **Dysphagia** (compressive symptom — present for 2 years, progressive) - **Tracheal deviation** on imaging - Benign FNAC (Bethesda Category II) - Normal thyroid function (euthyroid) ## Why Total Thyroidectomy is Correct **Key Point:** Surgery is the definitive treatment for benign MNG when **compressive symptoms are present**. This patient explicitly reports *progressive dysphagia* — a classic compressive symptom — along with radiological evidence of tracheal deviation, making observation inappropriate. **High-Yield Indications for Surgery in Benign MNG (Bailey & Love / Schwartz's Principles of Surgery):** 1. Compressive symptoms: dysphagia, dyspnea, stridor, hoarseness 2. Tracheal deviation with airway compromise 3. Cosmetic disfigurement (patient preference) 4. Suspicion of malignancy on FNAC 5. Toxic (hyperfunctioning) MNG 6. Retrosternal extension **Why Total Thyroidectomy over Hemithyroidectomy?** - The goiter is **multinodular and bilateral** in nature (multinodular goiter implies diffuse glandular involvement) - Hemithyroidectomy alone carries a high recurrence rate (~40–60% over 10 years) in bilateral MNG - Total thyroidectomy eliminates recurrence risk and is the preferred operation for symptomatic bilateral MNG (Schwartz's Principles of Surgery, 11th ed.) ## Why Other Options Are Incorrect | Option | Reason Incorrect | |--------|-----------------| | **Observation** | Compressive symptoms (dysphagia) are present — observation is inappropriate | | **Radioactive Iodine (RAI)** | Reserved for toxic MNG or post-surgical remnant; not first-line for euthyroid compressive MNG; slow response and may worsen swelling acutely | | **Right hemithyroidectomy + isthmectomy** | Inadequate for bilateral MNG; high recurrence risk; does not address left lobe disease | ## Management Algorithm for Symptomatic Benign MNG ``` Benign MNG on FNAC ↓ Compressive symptoms present? (Dysphagia ✓, Tracheal deviation ✓) ↓ YES → Total Thyroidectomy (preferred) → Lifelong levothyroxine replacement post-operatively ``` **Clinical Pearl:** Tracheal deviation *combined* with dysphagia constitutes clear surgical indication. The progressive nature of symptoms over 2 years further supports operative intervention rather than watchful waiting. Post-operatively, patients require lifelong thyroxine replacement (Bailey & Love's Short Practice of Surgery, 27th ed.). **High-Yield:** For NEET PG/INI-CET — symptomatic MNG (dysphagia, dyspnea, stridor) = Total thyroidectomy. Asymptomatic euthyroid MNG with benign FNAC = Observation. 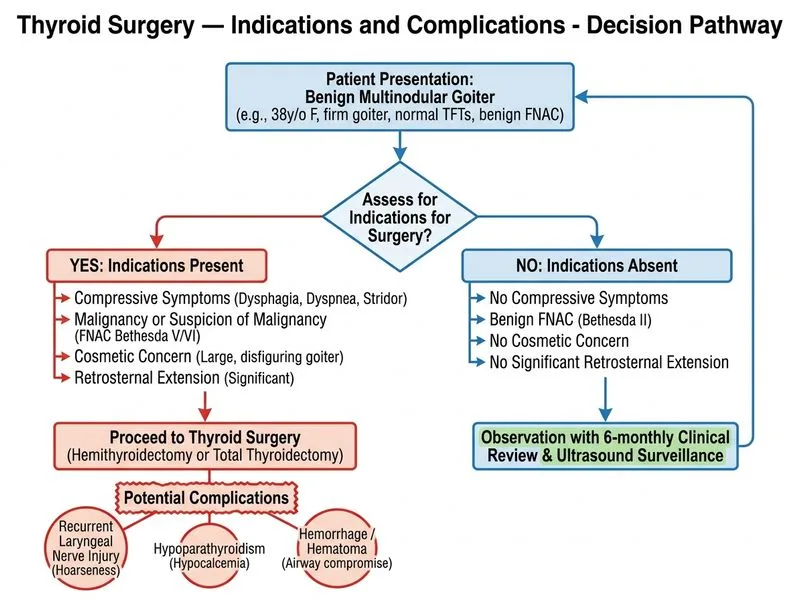
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.