## Clinical Assessment This patient has a **compressive multinodular goiter** with objective airway compromise (tracheal narrowing to 8 mm, stridor, dysphagia) and benign cytology. The presence of substernal extension (thoracic inlet involvement on CT) indicates the need for definitive surgical intervention. **Key Point:** Symptomatic goiter with significant tracheal compression (< 10 mm diameter) is an absolute indication for thyroidectomy, regardless of TSH or cytology findings. ## Indications for Thyroid Surgery in Goiter | Indication | Management | |---|---| | **Compressive symptoms** (stridor, dysphagia, dyspnea) | Thyroidectomy ± sternotomy | | **Tracheal compression** (< 10 mm on imaging) | Thyroidectomy ± sternotomy | | **Substernal extension** | Extended cervical approach ± sternotomy | | **Euthyroid goiter, asymptomatic** | Observation or TSH suppression | | **Malignancy suspected** (FNAC: suspicious/malignant) | Thyroidectomy ± neck dissection | ## Why Total Thyroidectomy with Sternotomy? 1. **Tracheal compression (8 mm)** — below the critical threshold; risk of intraoperative airway loss during dissection of upper poles 2. **Substernal extension** — lower poles extend into thoracic inlet; standard cervical approach may not provide adequate mobilization and hemostasis 3. **Sternotomy** — allows safe division of lower poles under direct visualization, reduces risk of recurrent laryngeal nerve injury and hemorrhage **Clinical Pearl:** In substernal goiter with severe compression, sternotomy is NOT routine but should be anticipated and the patient counseled preoperatively. Median sternotomy provides excellent exposure of the lower poles and mediastinal extension. **High-Yield:** The decision for sternotomy is made **intraoperatively** if the lower poles cannot be safely delivered into the neck or if vascular compromise is evident. However, in this case, preoperative counseling and preparation are essential. ## Why Not the Other Options? - **Levothyroxine suppression:** TSH is already normal (euthyroid goiter); suppression therapy has no role in symptomatic, compressive goiter. It may slow growth but will not relieve airway obstruction. - **Subtotal thyroidectomy:** Leaves residual thyroid tissue; higher recurrence rate (up to 10–15%) in multinodular disease. In compressive goiter, total thyroidectomy is preferred to eliminate recurrence risk and future re-operation. - **Observation:** Contraindicated in symptomatic, compressive disease. Stridor and dysphagia indicate hemodynamic airway compromise; risk of acute airway loss during anesthesia induction. **Mnemonic: STITCH** — **S**ymptoms (stridor, dysphagia), **T**racheal compression (< 10 mm), **I**maging substernal, **T**otal thyroidectomy, **C**onsider **H**elp (sternotomy). 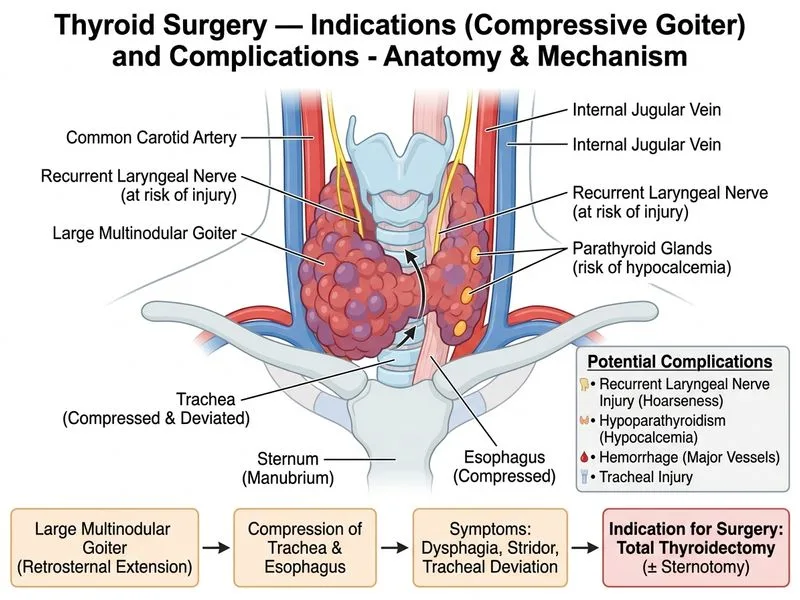
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.