## Postoperative RLN Injury: Mechanism and Management **Key Point:** Postoperative vocal cord paralysis in the paramedian position indicates **neurapraxia** (nerve conduction block) rather than complete transection. The paramedian position reflects unopposed cricothyroid action (superior laryngeal nerve intact) with loss of posterior cricoarytenoid function (RLN-innervated). ## Classification of RLN Injury | Injury Type | Mechanism | Vocal Cord Position | Prognosis | Management | |---|---|---|---|---| | **Neurapraxia** | Traction, compression, thermal injury (< 60°C) | Paramedian | Excellent (90–95% recovery) | Observation + voice therapy × 3–6 months | | **Axonotmesis** | Moderate thermal injury (60–70°C), crushing | Paramedian initially, may drift lateral | Good (6–12 months) | Voice therapy; consider reinnervation if no recovery by 12 months | | **Neurotmesis** | Complete transection, severe thermal injury (> 70°C) | Lateral (cadaveric) | Poor without repair | Urgent exploration + primary repair or grafting | ## Why Neurapraxia in This Case? 1. **Paramedian position** — indicates intact cricothyroid (innervated by superior laryngeal nerve, external branch) with loss of posterior cricoarytenoid (RLN-innervated). This is the classic position in neurapraxia. 2. **Surgeon identified and dissected RLN** — suggests the nerve was visualized and preserved; no evidence of transection. 3. **Immediate postoperative onset** — consistent with traction, retraction, or thermal injury causing conduction block, not axonal degeneration (which takes 3–5 days). 4. **Excellent prognosis for recovery** — 90–95% of neurapraxia cases recover spontaneously within 3–6 months as edema resolves and nerve conduction recovers. **Clinical Pearl:** The **paramedian position is reassuring** — it indicates the nerve is intact and conducting some impulses (superior laryngeal nerve). Complete transection would result in a **lateral (cadaveric) position** with loss of both RLN and superior laryngeal nerve function. ## Management Algorithm ```mermaid flowchart TD A[Postoperative vocal cord paralysis]:::outcome --> B{Vocal cord position?}:::decision B -->|Paramedian| C[Neurapraxia likely]:::outcome B -->|Lateral| D[Neurotmesis likely]:::outcome C --> E[Voice therapy + observation × 3-6 months]:::action E --> F{Recovery by 6 months?}:::decision F -->|Yes| G[Complete recovery]:::outcome F -->|No| H[Consider reinnervation at 12 months]:::action D --> I[Urgent surgical exploration]:::urgent I --> J[Primary repair or nerve graft]:::action ``` **High-Yield:** Do NOT rush to re-explore for paramedian paralysis. The majority recover spontaneously. Exploration is reserved for **lateral position** (transection) or **no recovery after 12 months** (consider reinnervation: ansa cervicalis transfer, nerve graft). ## Why Not the Other Options? - **Immediate voice therapy alone (Option 1):** Correct management but the mechanism is not thermal injury; neurapraxia is more likely given the paramedian position and surgeon's careful dissection. - **Urgent surgical exploration (Option 2):** Contraindicated in paramedian position. Exploration risks further nerve damage and is reserved for lateral position (transection) or confirmed neurotmesis. Paramedian paralysis has excellent prognosis with conservative management. - **No intervention (Option 4):** Incorrect; voice therapy is essential to prevent vocal cord atrophy and maintain voice quality during recovery. Also, tumor invasion would present preoperatively; this is iatrogenic injury. **Mnemonic: PARA-MEDIAL** — **P**aramedian position, **A**lmost always neurapraxia, **R**ecovery excellent (90–95%), **A**void re-exploration, **M**anage conservatively, **E**xpect recovery in 3–6 months, **D**iscuss voice therapy, **I**f no recovery at 12 months, consider reinnervation, **A**lways counsel patient, **L**ateral position = transection (explore). 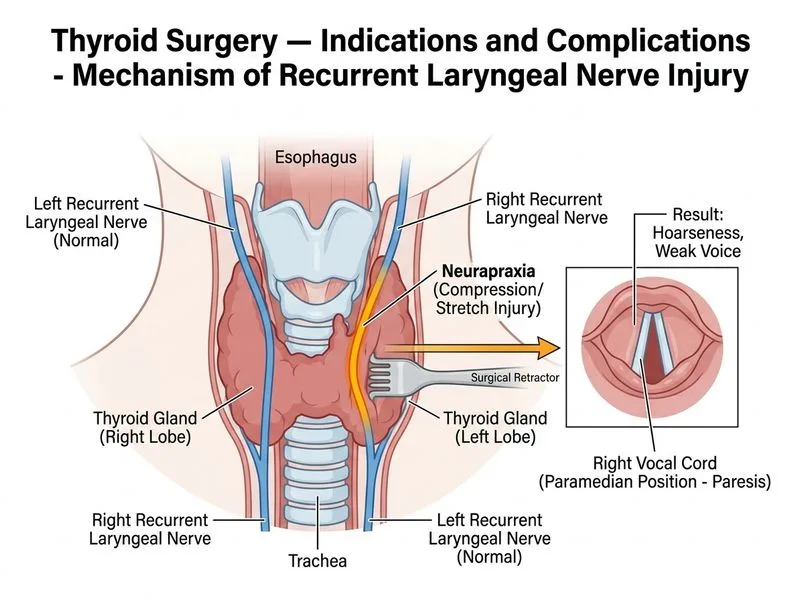
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.