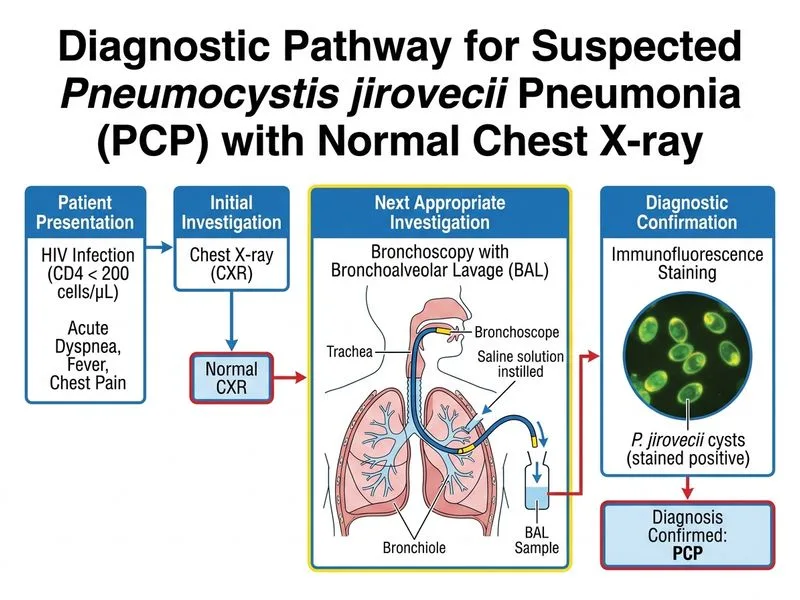
A 28-year-old woman with known HIV infection (CD4 count 85 cells/µL) presents with acute dyspnea, fever, and chest pain. Chest X-ray is normal. She is suspected of having Pneumocystis jirovecii pneumonia (PCP). What is the most appropriate next investigation to confirm the diagnosis?
A. High-resolution CT chest with prone imaging
B. Sputum induction with Giemsa staining
C. Bronchoscopy with bronchoalveolar lavage and immunofluorescence staining
D. Chest X-ray with prone positioning and expiratory views
Explanation
Confirmatory Investigation for PCP in Advanced HIV
Key Point
Bronchoscopy with bronchoalveolar lavage (BAL) and immunofluorescence staining (or Giemsa/Wright-Giemsa stain) is the gold standard for confirming Pneumocystis jirovecii pneumonia (PCP), especially when clinical suspicion is high and non-invasive tests are inconclusive.
Why BAL is Superior in This Case
Sensitivity and specificity:
BAL with immunofluorescence: >95% sensitivity and specificity for PCP
Sputum induction: Only 50–80% sensitivity; lower yield in advanced immunosuppression
Direct visualization: Allows assessment of airway involvement and exclusion of other opportunistic infections (CMV, mycobacteria, fungi)
Diagnostic Algorithm for Suspected PCP
Loading diagram...
Comparison of Diagnostic Methods
Table
Method
Sensitivity
Specificity
Invasiveness
Turnaround
Use Case
CXR (standard)
75–85%
High
Non-invasive
Immediate
Screening; normal CXR does NOT exclude PCP
CXR (prone/expiratory)
85–90%
High
Non-invasive
Immediate
Improves detection of early/subtle infiltrates
HRCT (prone)
95–98%
High
Non-invasive
Minutes
Excellent for detecting early PCP; may show ground-glass opacities
Sputum induction
50–80%
High
Minimally invasive
24 hrs
First-line in resource-limited settings; lower yield in advanced immunosuppression
BAL + immunofluorescence
>95%
>95%
Invasive
24 hrs
Gold standard; allows concurrent diagnosis of other infections
Clinical Pearl
In this patient with CD4 < 100 cells/µL, normal CXR does NOT exclude PCP. Up to 10–15% of PCP cases present with normal or near-normal chest imaging. BAL is indicated when clinical suspicion is high despite negative or equivocal non-invasive imaging.
High-YieldNEET PG
PCP prophylaxis is indicated when CD4 < 200 cells/µL (typically with TMP-SMX). If this patient is not on prophylaxis, PCP is a likely diagnosis and BAL confirmation is essential before starting therapy.
Mnemonic
BAL-IF = Bronchoscopy Alveolar Lavage with Immunofluorescence = gold standard for PCP.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.