| Feature | High Lesion | Low Lesion |
|---|---|---|
| Flexor carpi ulnaris (FCU) | Paralyzed (wrist flexion weak) | Intact (wrist flexion preserved) |
| Flexor digitorum profundus (FDP) to digits 4–5 | Paralyzed (DIP flexion lost) | Intact (DIP flexion preserved) |
| Intrinsic hand muscles | Paralyzed (claw hand) | Paralyzed (claw hand) |
| Claw hand pattern | Affects all 4 fingers (2–5) | Affects only digits 4–5 |
| Wrist flexion | Weak or absent | Normal |
| Sensory loss | Medial 1.5 digits + dorsal aspect | Medial 1.5 digits (palmar only) |
Froment's sign (thumb IP flexion when pinching paper) is positive in BOTH high and low lesions — it tests the adductor pollicis (ulnar-innervated), not a discriminator between levels.
Wartenberg's sign (abducted little finger) occurs in low lesions due to unopposed abductor digiti minimi; in high lesions, the entire hand is clawed, so the little finger is not simply abducted.
Loading illustration…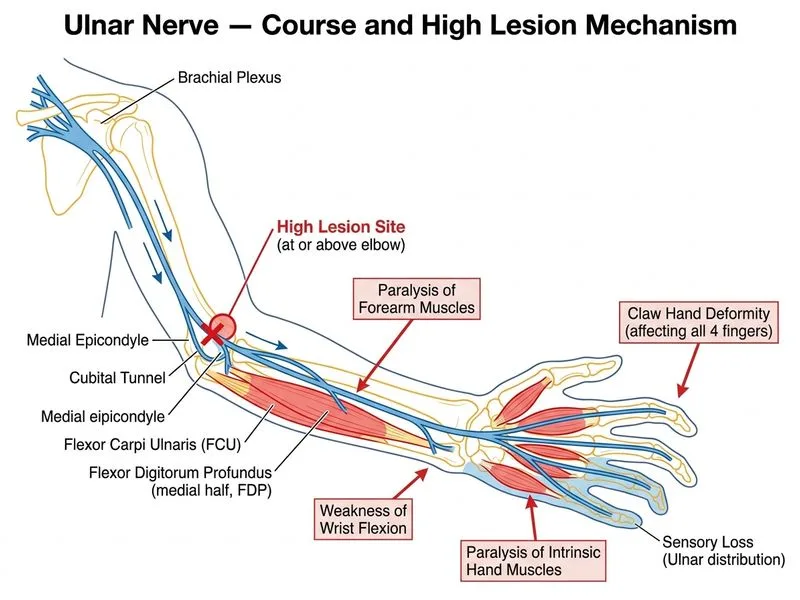
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →