A 58-year-old man from rural India presents with progressive dyspnea on exertion and orthopnea for 3 months. He has a history of acute rheumatic fever (ARF) at age 12. On examination, he has an irregular pulse (90 bpm), elevated JVP, hepatomegaly, and bilateral ankle edema. Auscultation reveals a loud S1, opening snap at the apex, and a low-pitched diastolic murmur best heard at the apex in the left lateral decubitus position. Chest X-ray shows pulmonary congestion and straightening of the left heart border. ECG shows atrial fibrillation with a ventricular rate of 92 bpm and left atrial enlargement. What is the most likely diagnosis?
A. Aortic regurgitation with left ventricular failure
B. Tricuspid stenosis with right ventricular failure
C. Mitral regurgitation with secondary atrial fibrillation
D. Mitral stenosis with atrial fibrillation
Explanation
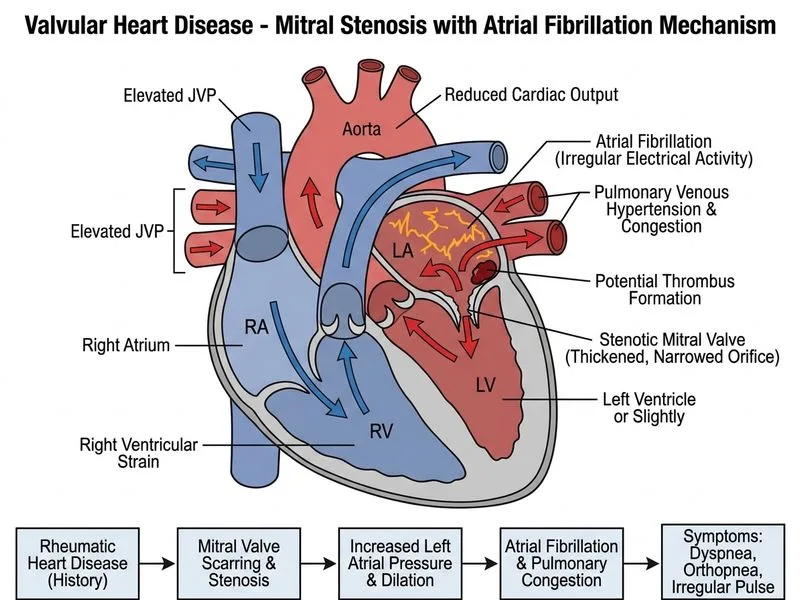
Clinical Diagnosis: Mitral Stenosis with Atrial Fibrillation
Key Clinical Features
Key Point
The combination of a loud S1, opening snap, and a low-pitched diastolic murmur at the apex in the left lateral decubitus position is pathognomonic for mitral stenosis (MS).
High-YieldNEET PG
Mitral stenosis is the most common valvular lesion resulting from rheumatic heart disease in India and developing countries. The opening snap occurs when the stenotic mitral valve leaflets abruptly stop their opening motion during early diastole.
Pathophysiology of Mitral Stenosis
1.
Valve pathology: Rheumatic damage causes commissural fusion, leaflet thickening, and calcification of the mitral valve.
2.
Hemodynamic consequence: Narrowed mitral orifice (normal area ~4–6 cm²; symptomatic MS typically <2 cm²) impedes left atrial emptying.
3.
Atrial enlargement: Chronic elevation of left atrial pressure causes left atrial dilation and fibrosis.
4.
Atrial fibrillation: Enlarged atrium becomes electrically unstable, leading to AF in 50–60% of symptomatic MS patients.
5.
Pulmonary congestion: Elevated LA pressure is transmitted retrograde to the pulmonary circulation, causing dyspnea, orthopnea, and pulmonary edema.
Diagnostic Findings in This Case
Table
Feature
Significance
Loud S1
Indicates mobile mitral valve leaflets; in severe stenosis with calcification, S1 becomes soft
Opening snap
High-pitched sound 60–150 ms after A2; earlier snap = more severe stenosis
Diastolic murmur
Low-pitched, rumbling; best heard with bell at apex in left lateral decubitus; increases with exercise or amyl nitrite (increases cardiac output)
Atrial fibrillation
Common complication; increases risk of thromboembolism (LA thrombus)
Pulmonary congestion on CXR
Reflects elevated LA pressure; straightening of left heart border = LA enlargement
Left atrial enlargement on ECG
Broad, notched P wave in lead II (P mitrale)
Why Atrial Fibrillation Develops
Clinical Pearl
AF in MS is a consequence of chronic LA enlargement and elevated LA pressure, not a primary arrhythmia. Once AF develops, the loss of atrial "kick" worsens hemodynamics and increases symptom severity.
Mnemonic: CHADS₂ Score — Congestive heart failure, Hypertension, Age ≥75, Diabetes, Stroke/TIA (×2). This patient has MS with AF and likely qualifies for anticoagulation.
Management Principles
1.
Rate control: Beta-blockers or calcium channel blockers to slow ventricular response in AF.
2.
Anticoagulation: Warfarin or DOAC for AF (high thromboembolic risk in MS).
3.
Diuretics: For pulmonary congestion and peripheral edema.
4.
Definitive treatment: Percutaneous mitral balloon commissurotomy (PMBC) if suitable anatomy, or surgical mitral valve replacement if severe, calcified, or failed PMBC.
Loading diagram...
Why This Patient Has MS, Not Other Lesions
Loud S1 and opening snap rule out aortic valve disease and severe mitral regurgitation (in MR, S1 is soft and there is no opening snap).
Diastolic murmur at apex is specific for MS; aortic regurgitation produces an early diastolic murmur at the left sternal border.
History of ARF is the strongest risk factor for MS in developing countries.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.