A 52-year-old woman from urban India presents with acute onset of severe dyspnea, hemoptysis, and syncope while climbing stairs. She has a 15-year history of mitral stenosis diagnosed after an episode of acute rheumatic fever. She denies chest pain. On examination, she is tachypneic (respiratory rate 32/min), cyanotic, and has a blood pressure of 95/60 mmHg. Auscultation reveals a loud S2, a prominent right ventricular heave, and a pulsatile hepatomegaly. Chest X-ray shows acute pulmonary edema with Kerley B lines and a prominent pulmonary artery. ECG demonstrates right axis deviation and right ventricular strain pattern. What is the most likely acute complication?
A. Acute left ventricular infarction with cardiogenic shock
B. Acute pulmonary embolism with right heart strain
C. Acute aortic dissection with hemodynamic collapse
D. Acute right ventricular failure secondary to pulmonary hypertension
Explanation
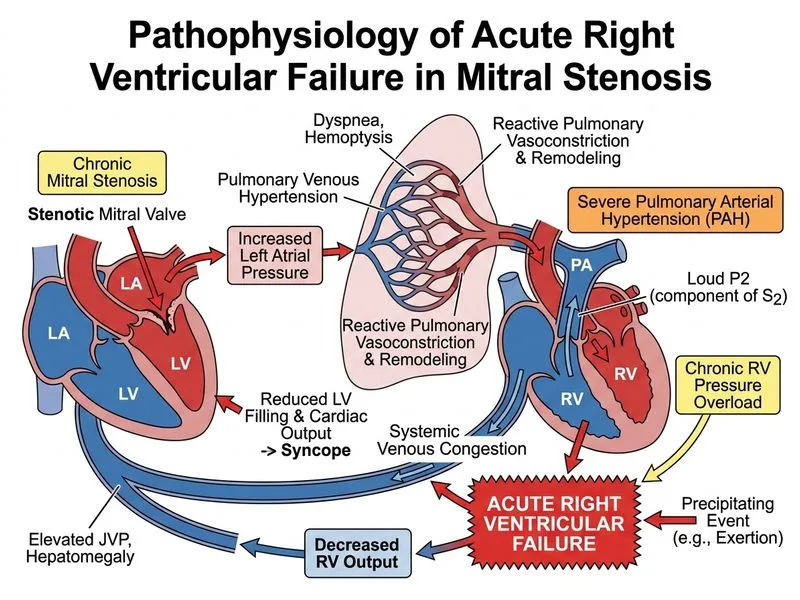
Acute Complication: Right Ventricular Failure Secondary to Pulmonary Hypertension
Pathophysiology of RV Failure in Mitral Stenosis
Key Point
Chronic mitral stenosis leads to progressive pulmonary hypertension, which ultimately causes right ventricular failure. This is a natural evolution of untreated MS and represents a critical hemodynamic decompensation.
Mechanism of Pulmonary Hypertension in MS
1.
Passive pulmonary hypertension (early): Elevated left atrial pressure is transmitted retrograde to the pulmonary circulation, increasing pulmonary venous and capillary pressures.
2.
Reactive pulmonary hypertension (progressive): Chronic pulmonary venous hypertension triggers pulmonary arteriolar vasoconstriction and medial hypertrophy of pulmonary arteries (muscularization).
3.
Fixed pulmonary hypertension (late): Structural remodeling of pulmonary vessels becomes irreversible; pulmonary vascular resistance remains elevated even after mitral valve surgery.
4.
RV pressure overload: The right ventricle must generate increasingly higher pressures to eject blood against the elevated pulmonary vascular resistance.
5.
RV dilatation and failure: Chronic RV pressure overload leads to RV hypertrophy, then dilatation, and eventually systolic dysfunction.
Clinical Features of Acute RV Failure in This Case
Table
Finding
Mechanism
Acute dyspnea & hemoptysis
Pulmonary edema from elevated LA pressure; hemoptysis from rupture of dilated bronchial veins or pulmonary infarction
Syncope on exertion
Inability of RV to increase cardiac output; fixed or falling systemic BP during increased demand
Acute decompensation with Kerley B lines (interlobular septal edema) and prominent pulmonary artery
Right axis deviation & RV strain on ECG
RV hypertrophy and acute RV pressure overload
Natural History of Untreated Mitral Stenosis
High-YieldNEET PG
The progression from MS → pulmonary hypertension → RV failure is a classic hemodynamic cascade. Exertion (which increases cardiac output and LA pressure) can precipitate acute decompensation.
Loading diagram...
Why Syncope Occurs
Clinical Pearl
Syncope in MS with pulmonary hypertension indicates severe RV dysfunction. The RV cannot increase cardiac output during exertion, leading to a paradoxical fall in systemic blood pressure and cerebral hypoperfusion. This is a sign of advanced disease and carries a poor prognosis without urgent intervention.
Immediate: Oxygen, diuretics, vasodilators (nitrates, hydralazine) to reduce LA pressure.
2.
Pulmonary vasodilators: Inhaled nitric oxide or sildenafil may provide temporary relief but do not reverse fixed pulmonary hypertension.
3.
Definitive: Urgent mitral valve replacement (PMBC is contraindicated in severe pulmonary hypertension with RV failure due to risk of acute decompensation).
Mnemonic: ARDS vs. Pulmonary Edema in MS — Acute Respiratory Distress Syndrome (ARDS) requires bilateral infiltrates and PEEP; pulmonary edema in MS shows Kerley B lines, cardiomegaly, and responds to diuretics.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.