A 52-year-old man with a history of acute rheumatic fever presents with a systolic ejection murmur at the right upper sternal border, radiating to the carotids. He has a narrow pulse pressure and a slow-rising carotid pulse. Chest X-ray shows a normal cardiac silhouette. Which investigation is most specific for confirming the diagnosis of aortic stenosis and assessing its hemodynamic severity?
A. Transthoracic echocardiography with Doppler
B. Electrocardiography
C. Exercise stress testing
D. Chest X-ray with barium swallow
Explanation
Diagnosis and Severity Assessment of Aortic Stenosis
Key Point
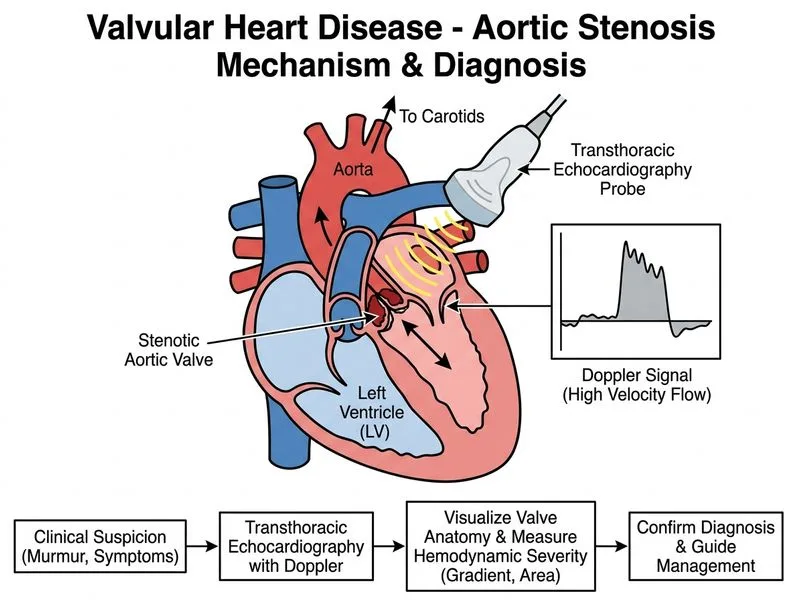
Transthoracic echocardiography with Doppler is the gold standard, most specific investigation for confirming aortic stenosis and quantifying its hemodynamic severity.
Why Transthoracic Echocardiography with Doppler?
1.
Direct visualization of the aortic valve — identifies:
Valve morphology (bicuspid, tricuspid, calcified)
Degree of valve opening and calcification
Left ventricular hypertrophy and function
2.
Quantifies hemodynamic severity using Doppler:
Peak aortic jet velocity (Vmax)
Peak systolic gradient (PSG)
Mean systolic gradient (MSG)
Aortic valve area (AVA) by continuity equation
3.
Guides management decisions — determines need for aortic valve replacement (surgical or transcatheter).
Severity Grading of Aortic Stenosis
Table
Parameter
Mild
Moderate
Severe
Vmax (m/s)
<3.0
3.0–4.0
>4.0
PSG (mmHg)
<36
36–64
>64
MSG (mmHg)
<25
25–40
>40
AVA (cm²)
>1.5
1.0–1.5
<1.0
High-YieldNEET PG
The continuity equation is the most accurate non-invasive method for calculating AVA:
AVA=AV VTILVOT area×LVOT VTI
Clinical Correlation with Physical Findings
Narrow pulse pressure and slow-rising carotid pulse (pulsus parvus et tardus) are classic signs of hemodynamically significant aortic stenosis, suggesting severe obstruction. Echocardiography quantifies this severity.
Role of Other Investigations
Electrocardiography — Shows:
Left ventricular hypertrophy (LVH) with strain pattern
Conduction abnormalities
NOT specific for aortic stenosis; non-diagnostic
Cannot assess severity or valve area
Chest X-ray — May show:
Aortic valve calcification ("aortic knob")
LVH (cardiomegaly)
NOT specific; cannot quantify severity
Normal CXR does not exclude significant AS
Exercise stress testing — Contraindicated in symptomatic aortic stenosis due to risk of syncope and sudden cardiac death. Used only in asymptomatic severe AS to assess for inducible symptoms.
Cardiac catheterization — Reserved for:
Coronary angiography (before valve replacement in older patients)
NOT first-line for diagnosis or severity assessment
Clinical Pearl
A patient with the classic triad of aortic stenosis (systolic ejection murmur at right upper sternal border, narrow pulse pressure, slow-rising pulse) requires echocardiography to confirm diagnosis and grade severity. This determines urgency of intervention and prevents sudden cardiac death from unrecognized severe AS.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.