This patient has symptomatic severe mitral regurgitation with reduced ejection fraction (EF 35%) and NYHA Class III symptoms despite optimal medical therapy with an ACE inhibitor and beta-blocker.
Symptomatic severe MR with EF ≤40% is a Class I indication for surgical intervention (valve repair or replacement), regardless of whether the patient is on maximal medical therapy. Medical management alone cannot prevent progressive ventricular dysfunction in severe organic MR.
Indications for surgery in mitral regurgitation:
| Indication | EF | Symptoms | Recommendation |
|---|---|---|---|
| Severe MR, primary (organic) | Any | Symptomatic | Surgery |
| Severe MR, primary | >60% | Asymptomatic | Surgery if EF declining or LA dilated |
| Severe MR, primary | ≤40% | Any | Surgery (Class I) |
| Severe MR, secondary (functional) | <30% | Symptomatic | Surgery + revascularization/CRT |
In primary (organic) MR due to structural valve disease, the regurgitant volume itself causes progressive LV dilatation and dysfunction. Surgery should not be delayed until EF falls further, as this worsens surgical outcomes and prognosis.
SEVERE MR + REDUCED EF = SURGERY
Referral for mitral valve repair/replacement is the standard of care because:
Harrison 21e Ch 282
Loading illustration…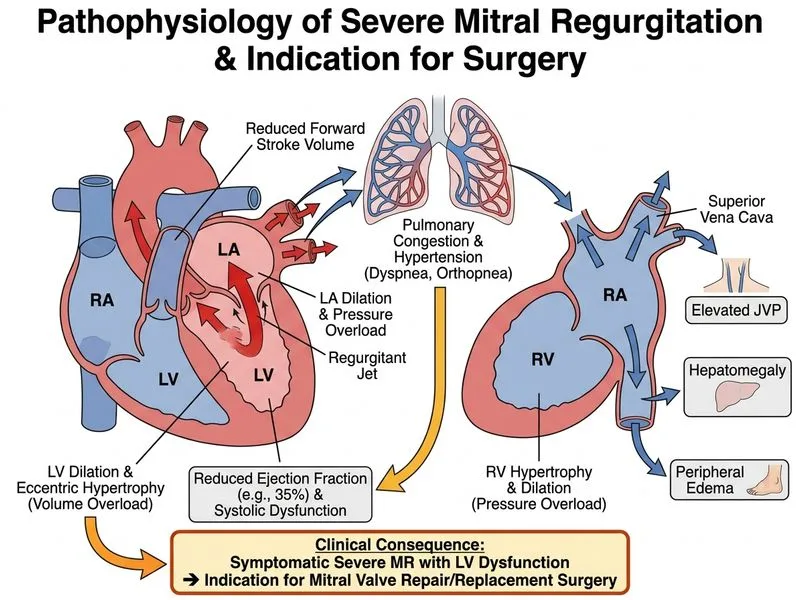
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →