This patient has symptomatic moderate-to-severe mitral stenosis (valve area 1.2 cm², mean gradient 18 mmHg) with normal sinus rhythm and no prior thromboembolism or documented left atrial thrombus.
Percutaneous mitral balloon valvotomy (PMBV) is the procedure of choice for symptomatic mitral stenosis with favorable valve anatomy and no contraindications. Anticoagulation strategy depends on individual thromboembolism risk factors, not solely on the decision to intervene.
Mitral Stenosis Management Algorithm:
| Feature | Favorable | Unfavorable |
|---|---|---|
| Valve area | <1.5 cm² | >1.5 cm² |
| Leaflet calcification | Absent/minimal | Extensive |
| Commissural fusion | Mild | Severe |
| Subvalvular disease | Minimal | Severe |
| Left atrial thrombus | Absent | Present |
| Mitral regurgitation | Mild | Moderate–severe |
This patient has:
Per ACC/AHA Valvular Heart Disease Guidelines and Harrison's Principles of Internal Medicine (21e, Ch. 282), warfarin anticoagulation in mitral stenosis is indicated when there is: (1) atrial fibrillation (paroxysmal, persistent, or permanent), (2) prior systemic thromboembolism, or (3) documented left atrial thrombus. This patient has none of these. In patients with normal sinus rhythm and no thromboembolism history, aspirin is appropriate for primary prevention and does not contraindicate PMBV. Warfarin is not indicated here because its bleeding risk outweighs benefit in the absence of established risk factors.
Warfarin is not indicated in this patient because:
While the left atrial diameter of 5.2 cm indicates LA enlargement (a risk factor for future AF), this alone does not constitute a current indication for warfarin per established guidelines. Anticoagulation is initiated when AF or thromboembolism is actually documented, not prophylactically for LA enlargement alone.
Beta-blockers are useful for rate control in AF or for symptom relief, but this patient is symptomatic with a valve area of 1.2 cm², which meets the threshold for intervention (≤1.5 cm²). Observation alone would be inappropriate when a definitive, low-risk intervention (PMBV) is available and indicated.
MVR is reserved for patients who are not candidates for PMBV — i.e., those with unfavorable valve anatomy (heavy calcification, severe subvalvular disease), significant mitral regurgitation, or left atrial thrombus not amenable to anticoagulation. PMBV is always the first-line intervention when anatomy is favorable, as it avoids the risks of open-heart surgery and prosthetic valve complications.
LA diameter >5.0 cm increases future AF risk and warrants close monitoring, but does not by itself mandate warfarin in a patient currently in sinus rhythm with no prior thromboembolism. Anticoagulation decisions must be based on current, documented indications — not anticipated future events.
Harrison 21e Ch 282; ACC/AHA 2021 Valvular Heart Disease Guidelines (Nishimura et al.)
Loading illustration…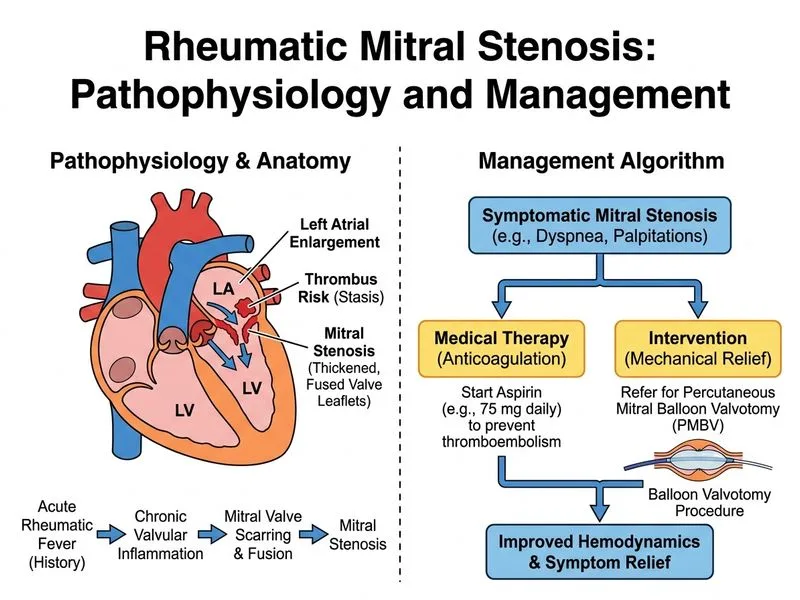
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →