In chronic mitral regurgitation, the left atrium and left ventricle gradually dilate over years, accommodating the regurgitant volume with less acute hemodynamic decompensation.
| Feature | Acute MR | Chronic MR |
|---|---|---|
| LV size | Normal or mildly enlarged | Markedly dilated |
| LA size | Normal or mildly enlarged | Markedly dilated |
| Pulmonary edema | Acute, severe (early) | Develops late, if at all |
| Atrial fibrillation | Uncommon (early) | Common (late) |
| Murmur character | Often soft, brief | Holosystolic, loud |
| CXR findings | Pulmonary edema + normal heart size | Cardiomegaly ± pulmonary edema |
Robbins 10e Ch 12
Loading illustration…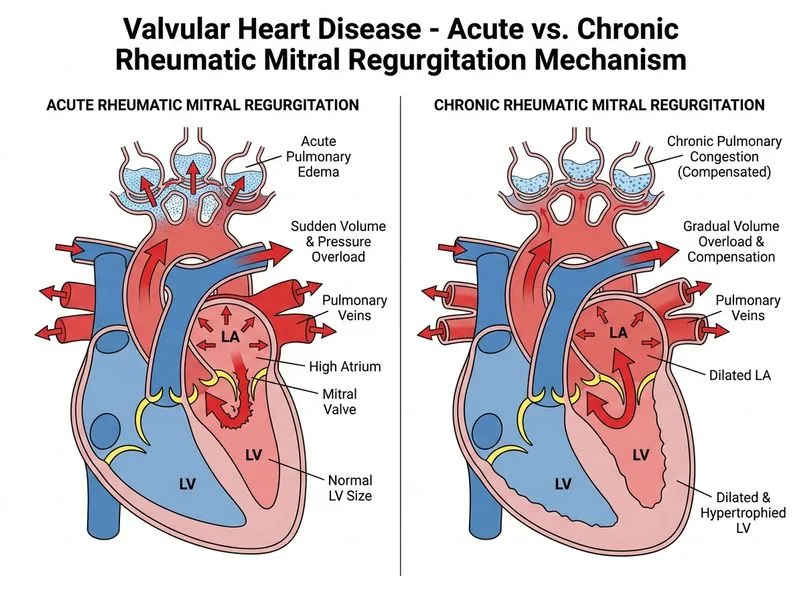
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →