## Superficial Thrombophlebitis Management This patient has **superficial thrombophlebitis (STP)** of the greater saphenous vein—a thrombotic inflammation of a superficial vein, distinct from deep vein thrombosis (DVT). ### Key Distinctions: - **STP** = inflammation + thrombosis of superficial veins (GSV, SSV) - **DVT** = thrombosis of deep veins (popliteal, femoral, iliac) - Duplex confirms **no deep venous involvement** → this is isolated STP ### Management of Isolated STP (No DVT): **Conservative management is standard:** - **Compression therapy** (class II–III stockings or bandaging) - **Leg elevation** to reduce swelling - **NSAIDs** (indomethacin 75 mg/day or ibuprofen) for pain and inflammation - **Early mobilization** to prevent stasis - **Anticoagulation is NOT routinely indicated** for isolated STP without DVT extension ### When Anticoagulation IS Considered: - STP **within 3 cm of the saphenofemoral junction** (risk of proximal extension to femoral vein) - **Concurrent DVT** (present in this case: NO) - **Malignancy-associated thrombophlebitis** (Trousseau syndrome) ### Why NOT Anticoagulation Here? - No DVT present - Greater saphenous vein involvement is distal from saphenofemoral junction - Risk of proximal extension is low with compression alone - ACCP guidelines (2016) recommend against routine anticoagulation for distal STP **High-Yield:** Superficial thrombophlebitis ≠ DVT. Isolated STP responds well to conservative measures; anticoagulation reserved for high-risk anatomy or DVT coexistence. 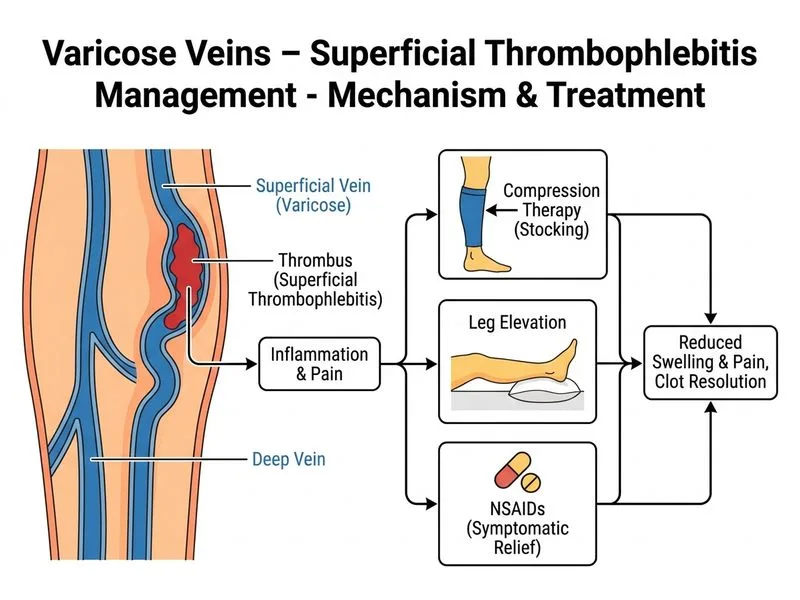
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.