A 58-year-old man from rural Maharashtra presents with a 3-week history of fever, malaise, and progressive dyspnea. On examination, he has a blood pressure of 165/95 mmHg, bilateral lower limb edema, and palpable purpura over the lower extremities and buttocks. Laboratory investigations show elevated ESR (95 mm/h), CRP 12 mg/dL, serum creatinine 2.8 mg/dL, and urinalysis reveals hematuria with RBC casts. Chest X-ray shows bilateral hilar infiltrates. Skin biopsy demonstrates leukocytoclastic vasculitis with IgA deposition on immunofluorescence. What is the most likely diagnosis?
A. IgA vasculitis (IgA nephropathy with systemic involvement)
B. Microscopic polyangiitis
C. Polyarteritis nodosa
D. Granulomatosis with polyangiitis
Explanation
Clinical Diagnosis: IgA Vasculitis
Key Clinical Features
Key Point
IgA vasculitis (formerly Henoch-Schönlein purpura) is the most common systemic vasculitis in children and young adults, characterized by IgA immune complex deposition in small vessels.
This patient presents with the classic tetrad:
1.
Palpable purpura — lower extremities and buttocks (pathognomonic distribution)
2.
Glomerulonephritis — hematuria with RBC casts, elevated creatinine
3.
Systemic symptoms — fever, malaise, dyspnea
4.
Skin biopsy confirmation — leukocytoclastic vasculitis with IgA deposition on immunofluorescence (gold standard)
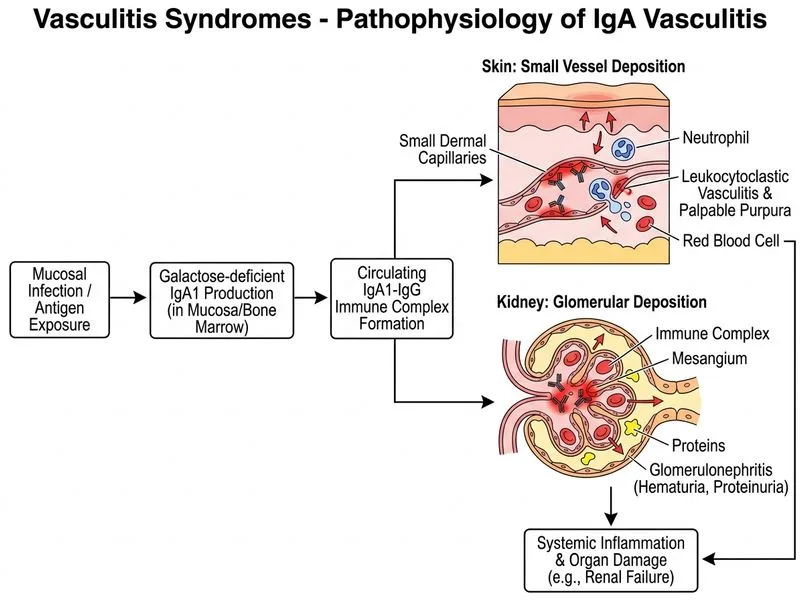
Pathophysiology
High-YieldNEET PG
IgA vasculitis is a small-vessel vasculitis mediated by IgA1-dominant immune complexes. The IgA deposition is the defining pathologic feature and distinguishes it from other small-vessel vasculitides.
Immunofluorescence Pattern
Table
Vasculitis Type
Immunofluorescence Pattern
Vessel Size
IgA vasculitis
IgA dominant
Small
Microscopic polyangiitis
ANCA (MPO or PR3)
Small
GPA
ANCA (PR3) + granulomas
Small–medium
PAN
Negative IF
Medium
Clinical Pearl
Clinical Pearl
The buttock and lower extremity purpura in a patient with concurrent glomerulonephritis and leukocytoclastic vasculitis is virtually pathognomonic for IgA vasculitis. The presence of IgA deposition on skin biopsy confirms the diagnosis.
Differential Consideration
Warning
Do not confuse with microscopic polyangiitis (which has ANCA positivity, no IgA deposition, and typically spares the skin) or GPA (which has granulomas and upper respiratory involvement).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.