A 62-year-old woman from Delhi presents with a 2-month history of progressive headache, jaw claudication, visual blurring, and temporal artery tenderness. On examination, she has a palpable, nodular, tender left temporal artery. ESR is 88 mm/h and CRP is 18 mg/dL. Temporal artery biopsy shows transmural inflammation with granulomatous infiltration and fragmentation of the internal elastic lamina. She also complains of morning stiffness in the shoulders and hips. What is the most likely diagnosis?
A. Behçet disease
B. Giant cell (temporal) arteritis with polymyalgia rheumatica
C. Polyarteritis nodosa
D. Takayasu arteritis
Explanation
Clinical Diagnosis: Giant Cell (Temporal) Arteritis with Polymyalgia Rheumatica
Key Clinical Features
Key Point
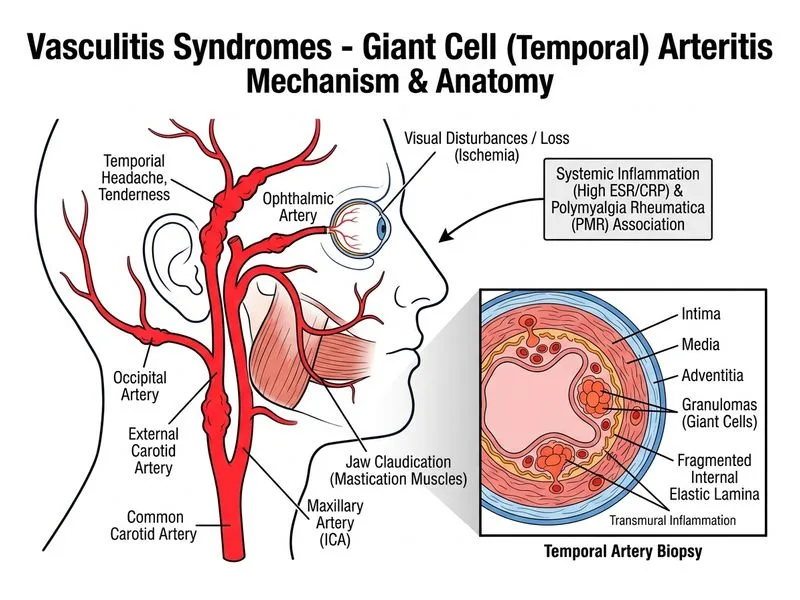
Giant cell arteritis (GCA) is a large-vessel vasculitis affecting the aorta and its branches, particularly the temporal and ophthalmic arteries. It is the most common vasculitis in patients >50 years of age.
Polymyalgia rheumatica — morning stiffness in shoulders and hips (present in ~50% of GCA patients)
Pathologic Hallmark
High-YieldNEET PG
Temporal artery biopsy showing transmural inflammation with granulomatous infiltration and fragmentation of the internal elastic lamina is the gold standard for diagnosis. This is a granulomatous vasculitis of large and medium vessels.
Diagnostic Algorithm
Loading diagram...
Temporal vs. Takayasu Arteritis
Table
Feature
Giant Cell Arteritis
Takayasu Arteritis
Age of onset
>50 years (typically 60–80)
<50 years (typically 10–40)
Ethnicity
Caucasian predominance
Asian, Indian, Latin American
Vessels affected
Temporal, ophthalmic, aortic arch
Aorta, subclavian, renal arteries
Presentation
Headache, jaw claudication, vision loss
Arm claudication, absent pulses
Polymyalgia rheumatica
Common (50%)
Rare
Biopsy finding
Granulomatous transmural inflammation
Granulomatous aortitis
Clinical Pearl
Clinical Pearl
Jaw claudication (pain in the jaw while chewing) is highly specific for temporal arteritis and should immediately raise suspicion. Visual symptoms (amaurosis fugax, diplopia, or permanent blindness) are ophthalmologic emergencies requiring urgent treatment with corticosteroids to prevent irreversible vision loss.
Management Urgency
Warning
Do not delay treatment while awaiting biopsy results if clinical suspicion is high. Corticosteroids should be initiated immediately to prevent vision loss, as the risk of blindness is ~15–20% if untreated. Biopsy can be performed within 1–2 weeks of starting steroids without significantly affecting diagnostic yield.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.