Vasculitis Syndromes MCQ — NEET PG Practice Question | NEETPGAI
Vasculitis Syndromes
medium
microscope Pathology
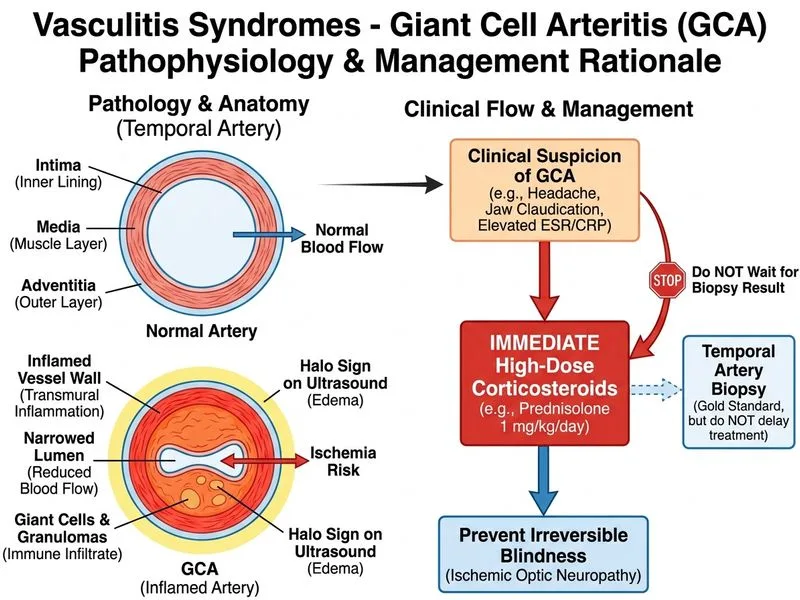
A 58-year-old man from Delhi presents with a 3-week history of fever, malaise, and progressive headache. Examination reveals temporal artery tenderness and jaw claudication. ESR is 92 mm/h and CRP is elevated. Temporal artery ultrasound shows a halo sign. What is the most appropriate next step in management?
A. Perform temporal artery biopsy before initiating any treatment
B. Start aspirin 75 mg daily and observe for 2 weeks with repeat ESR
C. Start prednisolone 1 mg/kg/day immediately without waiting for biopsy
D. Obtain CT angiography of the aorta to rule out aortic involvement
The clinical presentation is classic for GCA: elderly patient with temporal artery tenderness, jaw claudication, elevated inflammatory markers (ESR >90), and ultrasound halo sign (hallmark finding).
Management Priority
Key Point
In suspected GCA with clinical and imaging evidence of active disease, corticosteroid therapy must be initiated immediately to prevent irreversible vision loss from arteritic anterior ischemic optic neuropathy (AAION).
High-YieldNEET PG
The risk of permanent blindness in untreated GCA is 40–50% within weeks. Delay in treatment for biopsy confirmation is NOT acceptable when clinical suspicion is high and imaging is supportive.
Imaging confirmation: Halo sign on ultrasound is highly specific (95%) for GCA
3.
Threat to vision: Ophthalmic artery involvement can cause sudden, irreversible blindness
4.
Biopsy timing: Temporal artery biopsy can be performed after steroid initiation (within 1–2 weeks) without loss of diagnostic sensitivity if steroids have been given for <2 weeks
Clinical Pearl
The halo sign (hypoechoic ring around the temporal artery lumen on ultrasound) has replaced the need for immediate biopsy in many centers when clinical suspicion is high. Biopsy becomes confirmatory rather than gatekeeping.
Steroid Dosing
Induction: Prednisolone 1 mg/kg/day (typically 40–60 mg/day) for 2–4 weeks
Monitoring: ESR/CRP at 1–2 weeks; taper based on clinical response and inflammatory markers
Concurrent: PPI, calcium + vitamin D, and bisphosphonate for osteoporosis prophylaxis
Harrison 21e Ch 319
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.