| Feature | Giant Cell Arteritis | Takayasu Arteritis | Polyarteritis Nodosa | Behçet Disease |
|---|---|---|---|---|
| Age of onset | >50 years (elderly) | 10–40 years (young) | 40–60 years | 20–40 years |
| Vessel size | Medium–large (temporal, coronary, aorta) | Large (aorta, proximal branches) | Small–medium (renal, coronary) | Small–medium (veins, arteries) |
| Granulomatous inflammation | Yes (with giant cells) | Yes (with giant cells) | No (fibrinoid necrosis) | No (lymphocytic infiltrate) |
| Medial necrosis | Yes | Yes | Yes (fibrinoid) | No |
| Coronary involvement → MI | Yes (direct arteritis) | Ostial stenosis (less direct) | Occasional | Rare |
| Geography | Western countries; also Asia | Asia, Latin America | Worldwide | Mediterranean, Middle East, Asia |
This is identical to the histology described in the stem: granulomatous inflammation with giant cells and medial necrosis.
Giant Cell Arteritis can involve the coronary arteries directly, producing acute MI in the absence of atherosclerosis. The combination of:
…is pathognomonic for GCA affecting the coronary circulation.
Robbins 10e Ch 11; Harrison's Principles of Internal Medicine, 21e
Loading illustration…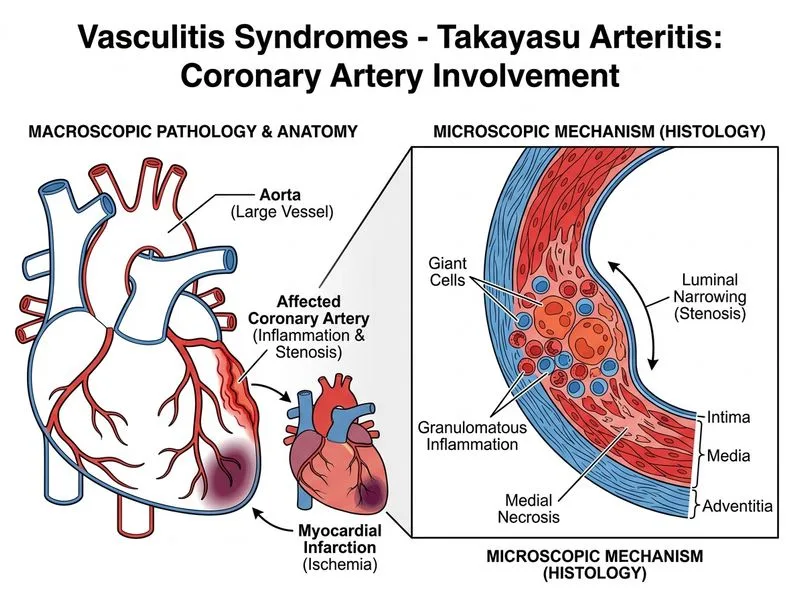
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →