Viral Keratitis MCQ — NEET PG Practice Question | NEETPGAI
Viral Keratitis
hard
eye Ophthalmology
A 28-year-old man presents with a 3-week history of right eye pain, photophobia, and progressive vision loss. He had a dendritic ulcer 2 months ago treated with topical acyclovir. On examination, visual acuity is 6/18. Slit-lamp biomicroscopy shows a dense, white, granular infiltrate in the corneal stroma with intact epithelium and anterior chamber reaction (3+ cells). Corneal sensation is normal. What is the most likely diagnosis and the appropriate next step in management?
A. HSV stromal keratitis; start topical prednisolone 1% 4 times daily plus oral acyclovir 400 mg 5 times daily
B. Bacterial keratitis; perform corneal scraping and culture, then start topical fortified antibiotics
C. Fungal keratitis; perform KOH mount and start topical natamycin 5%
D. Acyclovir-resistant HSV keratitis; switch to topical ganciclovir 0.15% 5 times daily
Explanation
Clinical Diagnosis: HSV Stromal Keratitis
Key Point
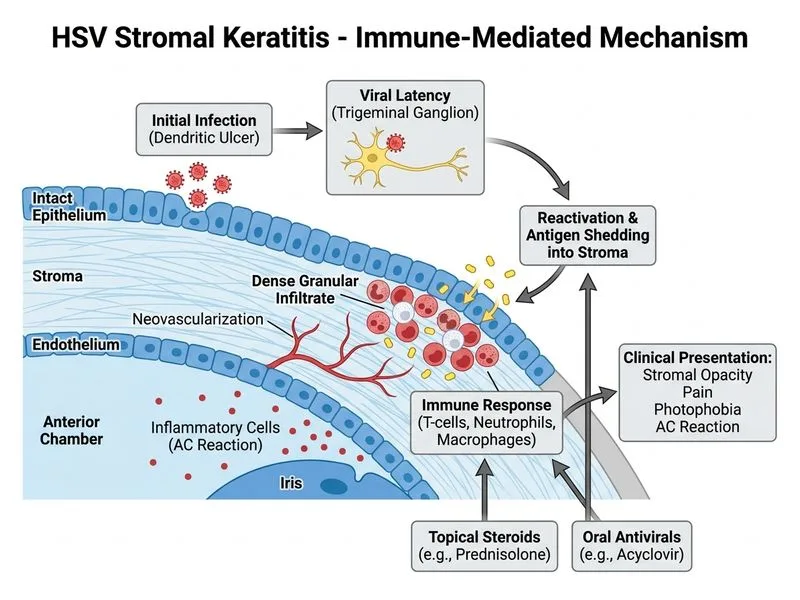
The history of prior dendritic ulcer, recurrent HSV infection, and stromal infiltration with intact epithelium indicates HSV stromal keratitis (HSK) — a delayed hypersensitivity immune response to viral antigen in the stroma, not active viral replication.
Pathophysiology of HSV Stromal Keratitis
Loading diagram...
Differential Diagnosis: Epithelial vs. Stromal HSV Keratitis
Table
Feature
Epithelial HSV
Stromal HSV (HSK)
Onset
Acute (days)
Subacute to chronic (weeks–months)
Ulcer Pattern
Dendritic or geographic
Intact epithelium
Stromal Involvement
Minimal
Dense infiltrates, neovascularization
Corneal Sensation
Reduced
Normal or near-normal
AC Reaction
Mild (0–1+)
Moderate to severe (2–4+)
Pathology
Active viral replication
Immune-mediated (Type III/IV hypersensitivity)
Treatment
Antivirals alone (acyclovir)
Antivirals + Topical Steroids
Prognosis
Good; heals in 7–10 days
Variable; risk of scarring & vision loss
High-YieldNEET PG
HSV stromal keratitis is an immune-mediated disease, not active viral infection. Therefore, steroids are NOT contraindicated — they are ESSENTIAL to suppress the inflammatory response. However, steroids MUST be combined with systemic antivirals to prevent epithelial reactivation.
Management of HSV Stromal Keratitis
Step 1: Confirm Diagnosis
History of prior HSV epithelial disease
Stromal infiltration with intact epithelium
Normal or near-normal corneal sensation (rules out active epithelial disease)
Anterior chamber reaction (immune response)
Step 2: Initiate Dual Therapy
Topical Prednisolone 1%:
Frequency: 4–6 times daily initially, taper over 4–6 weeks
Mechanism: Suppresses Type III/IV hypersensitivity and inflammatory cytokines
Efficacy: Reduces stromal edema and neovascularization
Oral Acyclovir 400 mg:
Frequency: 5 times daily for 10–14 days, then consider long-term prophylaxis (400 mg 2–3 times daily)
Mechanism: Prevents epithelial reactivation and viral shedding
Rationale: Steroids alone risk epithelial breakdown and geographic ulceration
Clinical Pearl
The combination of topical steroid + systemic antiviral is the cornerstone of HSK management. Steroids without antivirals lead to epithelial disease; antivirals without steroids fail to resolve stromal inflammation.
Step 3: Monitoring
Slit-lamp examination every 1–2 weeks
Monitor for epithelial breakdown (indicates need to reduce steroid dose)
Assess for stromal clearing and reduction in AC reaction
Long-term: Watch for corneal scarring and neovascularization
Why This Is NOT the Other Diagnoses
Bacterial Keratitis:
Bacterial keratitis presents with epithelial defect and suppurative infiltrate (not granular)
Rapid onset (24–48 hours) with severe pain
Corneal scraping would show bacteria on Gram stain
This patient has intact epithelium and prior HSV history — bacterial infection is unlikely
Fungal Keratitis:
Fungal keratitis is rare in immunocompetent hosts without risk factors (contact lens trauma, topical steroid abuse)
Presents with feathery infiltrate and satellite lesions
Slow progression over weeks to months
KOH mount would be negative in HSK
No mention of risk factors in this case
Acyclovir-Resistant HSV:
Rare in immunocompetent patients (<1% incidence)
Typically presents with recurrent epithelial disease, not stromal infiltration
Stromal disease in HSV is immune-mediated, not due to viral resistance
Switching to ganciclovir without steroids would fail to address the underlying immune pathology
Long-Term Management
Key Point
HSV stromal keratitis has a chronic course with risk of recurrence (up to 50% over 5 years). Long-term prophylaxis with oral acyclovir 400 mg 2–3 times daily reduces recurrence risk by ~50%.
Mnemonic: STEROID-ANTIVIRAL (S-A) Rule for HSK
S = Steroids (topical, tapered over weeks)
A = Antivirals (systemic, long-term prophylaxis)
Together they prevent both immune-mediated stromal damage and viral reactivation
Warning
Do NOT use steroids without antivirals in HSV disease — risk of epithelial breakdown and geographic ulceration. Do NOT use antivirals alone in HSK — stromal inflammation will persist.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.