Viral Keratitis MCQ — NEET PG Practice Question | NEETPGAI
Viral Keratitis
hard
eye Ophthalmology
A 45-year-old man with a history of recurrent HSV keratitis presents with stromal opacity, neovascularization, and anterior uveitis 3 weeks after onset of corneal symptoms. Topical acyclovir alone has been ineffective. What is the most appropriate next step in management?
A. Perform urgent corneal transplantation to prevent irreversible scarring
B. Switch to intravenous acyclovir 10 mg/kg 8-hourly for disseminated HSV infection
C. Discontinue acyclovir and initiate topical voriconazole for presumed fungal superinfection
D. Continue topical acyclovir and add topical prednisolone acetate 1% 4 times daily after epithelial healing is confirmed
Explanation
Clinical Diagnosis: HSV Stromal Keratitis
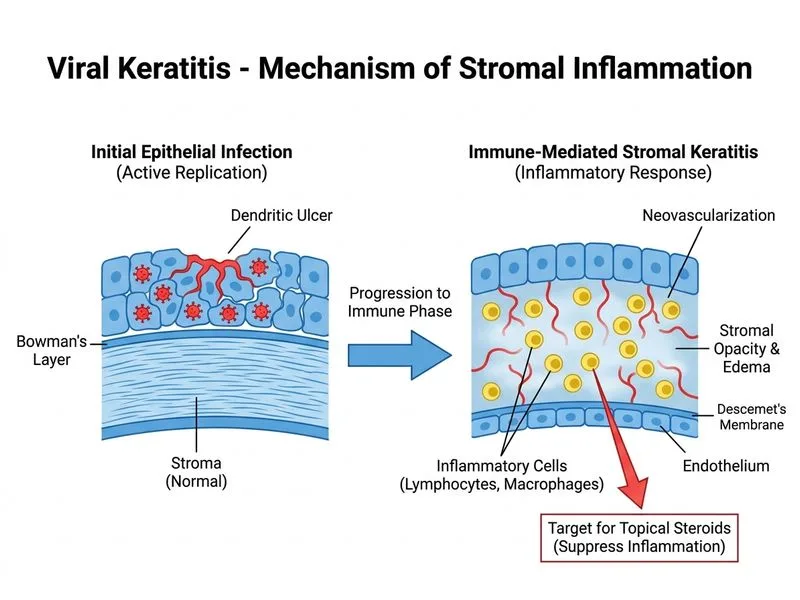
The progression from epithelial disease to stromal opacity, neovascularization, and anterior uveitis 3 weeks into illness indicates HSV stromal keratitis (HSK). This is an immune-mediated complication, not active viral replication.
Key Point
Stromal keratitis is a delayed hypersensitivity reaction to viral antigen, NOT active epithelial infection. Treatment shifts from antivirals alone to combination antiviral + topical steroid.
Pathophysiology of HSV Stromal Keratitis
Loading diagram...
Management of HSV Stromal Keratitis
High-YieldNEET PG
Topical steroids are ESSENTIAL in stromal HSK to suppress immune-mediated inflammation. They are contraindicated in epithelial disease but therapeutic in stromal disease.