Quick Answer
Autonomic pharmacology is a 3 to 5 question topic per NEET PG paper. Lock these:
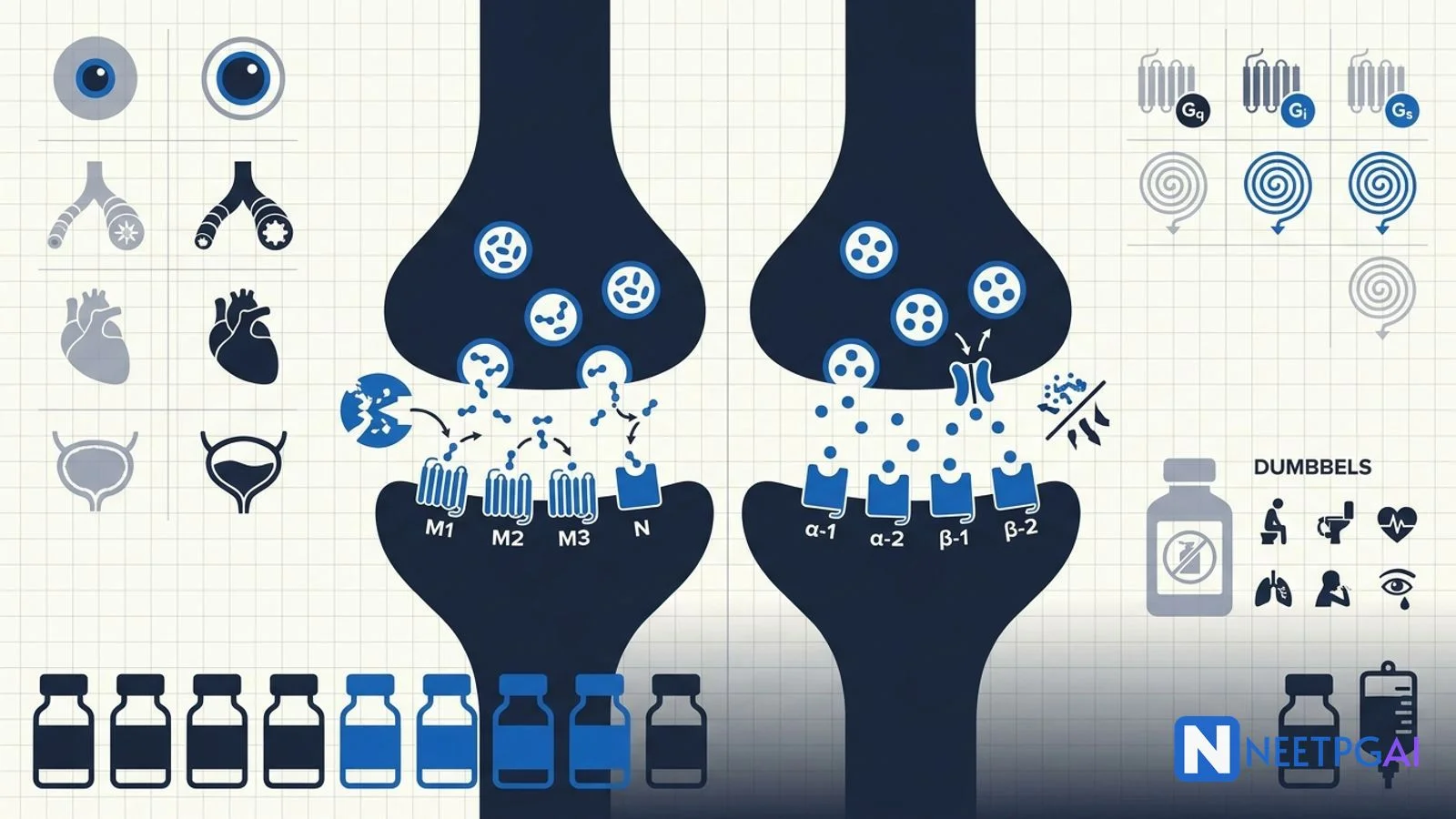
- Cholinergic crisis (DUMBBELS) — Defecation, Urination, Miosis, Bradycardia, Bronchospasm, Emesis, Lacrimation, Salivation.
- OP poisoning — atropine + pralidoxime within 24 h (before AChE-OP ageing).
- Receptor coupling — M1, M3, M5, alpha-1 = Gq (IP3/Ca); M2 = Gi; beta-1/2/3 = Gs (cAMP); alpha-2 = Gi.
- Beta-1 selective — Atenolol, Metoprolol, Bisoprolol, Esmolol, Nebivolol ("A-BEAM-N").
- Pheochromocytoma — phenoxybenzamine (alpha first) then beta-blocker.
- Donepezil, rivastigmine, galantamine — Alzheimer disease.
- Pyridostigmine — myasthenia gravis.
Autonomic pharmacology is the highest-volume topic on the pharmacology paper and the busiest overlap with internal medicine (CHF, HTN, asthma, COPD, glaucoma, BPH), psychiatry (ADHD, PTSD nightmares), and forensic medicine (OP suicide — accounting for ~one-third of all suicide deaths in India). Lock the receptor → signalling → drug → indication → adverse effect chain for every class and you have a high-yield 4 to 6 question domain locked.
This NEETPGAI deep dive covers cholinergic agonists/antagonists, adrenergic agonists/antagonists, the receptor coupling table, organophosphate poisoning (India context), and the high-yield MCQ traps. Pair this with the GI physiology guide for ANS control of GI smooth muscle.
Receptor families and coupling
| Receptor | G-protein | Second messenger | Major location |
|---|
| M1 | Gq | IP3, DAG, Ca2+ | CNS, gastric parietal cell |
| M2 | Gi | ↓ cAMP | Cardiac (SA, AV node) |
| M3 | Gq | IP3, DAG, Ca2+ | Smooth muscle, glands |
| M5 | Gq | IP3, DAG | CNS |
| Nicotinic-N (Nn) | Ligand-gated cation | — | Autonomic ganglia, adrenal medulla |
| Nicotinic-M (Nm) | Ligand-gated cation | — | Skeletal muscle NMJ |
| Alpha-1 | Gq | IP3, DAG | Vascular smooth muscle, prostate, bladder neck |
| Alpha-2 | Gi | ↓ cAMP | Presynaptic CNS/sympathetic (negative feedback), pancreatic beta cell |
| Beta-1 | Gs | ↑ cAMP | Heart (SA, AV, ventricle), JGA (renin) |
| Beta-2 | Gs | ↑ cAMP | Bronchi, uterus, skeletal-muscle vasculature, liver |
| Beta-3 | Gs | ↑ cAMP | Adipose tissue (lipolysis), bladder detrusor |
| D1 | Gs | ↑ cAMP | Renal arterioles, smooth muscle |
| D2 | Gi | ↓ cAMP | Nigrostriatal, pituitary (inhibits prolactin) |
Mnemonic for Gq: "HAVe 1 M&M" — H1, Alpha-1, V1, M1, M3.
Cholinergic agonists
Direct
- Pilocarpine — M3 agonist; topical for glaucoma, oral for Sjögren xerostomia.
- Bethanechol — M3 agonist; postoperative urinary retention, neurogenic bladder.
- Methacholine — methacholine challenge test for asthma.
- Carbachol — both M and N; intraoperative miosis in cataract surgery.
- Nicotine, varenicline — Nn agonists; smoking cessation.
Indirect (acetylcholinesterase inhibitors)
| Drug | Duration | Major use |
|---|
| Edrophonium | Ultra-short | Old Tensilon test (now obsolete) |
| Neostigmine | Short | Reversal of non-depolarising NMB; myasthenia gravis (with glycopyrrolate to block muscarinic effects) |
| Pyridostigmine | Long (4 to 6 h) | Myasthenia gravis chronic therapy |
| Physostigmine | Crosses BBB | Atropine poisoning, glaucoma (rare) |
| Donepezil, rivastigmine, galantamine | Long | Alzheimer disease |
| Organophosphates (parathion, malathion, sarin) | Irreversible | Pesticides, nerve agents — toxicology only |
Cholinergic antagonists
Muscarinic
- Atropine — non-selective; bradycardia (peri-arrest, OP poisoning), pre-anaesthesia, OP poisoning, mydriatic for fundoscopy (long-acting; tropicamide is preferred for shorter duration).
- Glycopyrrolate — quaternary (no BBB crossing); pre-anaesthesia drying of secretions, OP adjunct.
- Scopolamine — motion sickness (transdermal patch behind ear).
- Ipratropium, tiotropium — inhaled; COPD bronchodilation. Tiotropium is once-daily long-acting.
- Oxybutynin, tolterodine, solifenacin — overactive bladder (detrusor M3 block).
- Hyoscine butylbromide (Buscopan) — antispasmodic; renal/biliary colic, IBS.
- Benztropine, trihexyphenidyl — Parkinson tremor; drug-induced parkinsonism.
- Pirenzepine — selective M1; PUD (now obsolete).
Atropine toxidrome
"Hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter, full as a flask" — hyperthermia, anhidrosis, flushing, mydriasis, delirium, urinary retention. Treat with physostigmine (crosses BBB).
Nicotinic antagonists
- Ganglion blockers — hexamethonium, mecamylamine (historical; not used now).
- Neuromuscular blockers (Nm) — non-depolarising (atracurium, vecuronium, rocuronium — reversal with neostigmine + glycopyrrolate, or sugammadex for rocuronium/vecuronium); depolarising (succinylcholine — causes fasciculations, malignant hyperthermia risk, hyperkalaemia).
Organophosphate poisoning — India focus
Organophosphates and carbamates are irreversible AChE inhibitors. They cause both muscarinic and nicotinic features.
Features (DUMBBELS + nicotinic)
- Muscarinic: Defecation, Urination, Miosis, Bradycardia, Bronchospasm/Bronchorrhoea, Emesis, Lacrimation, Salivation.
- Nicotinic: muscle fasciculations → paralysis (including diaphragm), tachycardia (transient), hypertension.
- CNS: seizures, coma, respiratory depression.
Diagnosis
Clinical + low red-cell or plasma cholinesterase. Reduced plasma butyrylcholinesterase is more sensitive but less specific.
Management
- Decontamination — remove clothes, wash skin, gastric lavage if recent ingestion.
- Airway + ventilation — many die from secretions and diaphragmatic paralysis.
- Atropine — start 2 to 4 mg IV; double every 5 min until "atropinised" (dry mouth, clear chest, HR > 80, SBP > 90, pupils mid-position). Maintain infusion.
- Pralidoxime (2-PAM) — 1 to 2 g IV over 30 min, then infusion. Reactivates AChE by removing the OP. Effective only within ~24 h, before "ageing" (irreversible covalent stabilisation).
- Supportive — benzodiazepines for seizures, ICU monitoring.
Carbamates (e.g., physostigmine, pyridostigmine, carbaryl) cause similar features but are reversible — atropine alone is usually sufficient; pralidoxime is NOT routinely given.
Indian epidemiology
India accounts for about one-third of global OP suicide deaths (~50,000 to 60,000 per year), driven by agrarian distress and easy household pesticide access. Ban of WHO Class I OPs (parathion, methyl parathion, monocrotophos) and rollout of safer storage practices are public-health priorities.
Adrenergic agonists
Selective
| Drug | Receptor | Use |
|---|
| Phenylephrine | Alpha-1 | Decongestant, hypotension |
| Clonidine, methyldopa, dexmedetomidine | Alpha-2 (central) | HTN, opioid withdrawal, sedation; methyldopa in pregnancy |
| Dobutamine | Beta-1 | Cardiogenic shock, stress echo |
| Salbutamol, terbutaline | Beta-2 | Acute asthma, tocolysis |
| Salmeterol, formoterol | Long-acting beta-2 | COPD, asthma maintenance |
| Mirabegron | Beta-3 | Overactive bladder |
Non-selective
- Adrenaline (epinephrine) — alpha + beta; anaphylaxis (IM 0.5 mg), cardiac arrest (IV 1 mg every 3 to 5 min), local anaesthetic vasoconstrictor.
- Noradrenaline (norepinephrine) — predominantly alpha-1 + beta-1; septic shock vasopressor of choice.
- Dopamine — dose-dependent: low (D1 renal), intermediate (beta-1), high (alpha-1); now largely replaced by noradrenaline for shock.
- Isoprenaline — beta-1 + beta-2; bradyarrhythmias.
- Cocaine — blocks NA reuptake; sympathomimetic features (mydriasis, hypertension, tachycardia, MI).
- Amphetamine, methamphetamine — release NA + dopamine; ADHD (Adderall), narcolepsy.
- Tyramine — releases NA from vesicles; "cheese reaction" with MAOIs.
Adrenergic antagonists
Alpha
- Non-selective — phenoxybenzamine (irreversible, used preoperatively for pheochromocytoma); phentolamine (reversible, short-acting; hypertensive emergency in pheo, extravasation of vasopressors).
- Alpha-1 selective — prazosin (PTSD nightmares, resistant HTN), terazosin, doxazosin (HTN + BPH); tamsulosin and silodosin (uroselective alpha-1A — BPH).
Beta
| Drug | Selectivity | Notes |
|---|
| Atenolol, metoprolol, bisoprolol | Beta-1 selective | HTN, post-MI, CHF (bisoprolol) |
| Esmolol | Beta-1, ultra short-acting | IV intra-op |
| Nebivolol | Beta-1 + vasodilation (NO release) | HTN with metabolic benefit |
| Propranolol | Non-selective | Migraine prophylaxis, essential tremor, thyrotoxicosis, anxiety, portal HTN |
| Timolol | Non-selective | Topical for glaucoma |
| Sotalol | Non-selective + Class III antiarrhythmic | Refractory arrhythmias |
| Carvedilol | Alpha-1 + non-selective beta | Heart failure |
| Labetalol | Alpha-1 + non-selective beta | Hypertensive emergency, pregnancy HTN |
Pheochromocytoma — order matters
Phenoxybenzamine (alpha-blockade) FIRST for 10 to 14 days, THEN beta-blocker. If beta blocked first, unopposed alpha causes hypertensive crisis.
MAO and COMT inhibitors
- MAO-A — deaminates serotonin, NA, dopamine, tyramine. MAO-A inhibitors: moclobemide (reversible, safer with cheese), selegiline at high doses.
- MAO-B — deaminates dopamine selectively. MAO-B inhibitors: selegiline (low dose), rasagiline, safinamide — Parkinson disease adjuncts; no cheese reaction at low dose.
- COMT inhibitors — entacapone, tolcapone — prolong levodopa action in Parkinson.
NEET PG MCQ traps
- OP poisoning — atropine + pralidoxime within 24 h before ageing.
- Atropine toxidrome — anti-cholinergic — treat with physostigmine.
- Pheochromocytoma — phenoxybenzamine FIRST, then beta-blocker.
- Methyldopa — alpha-2 central agonist; HTN drug of choice in pregnancy (along with labetalol, nifedipine).
- Tamsulosin — alpha-1A uroselective; BPH; less postural hypotension.
- Beta-1 selective mnemonic — A-BEAM-N (Atenolol, Bisoprolol, Esmolol, Acebutolol, Metoprolol, Nebivolol).
- Propranolol — non-selective; contraindicated in asthma; useful in migraine, essential tremor, thyrotoxicosis, portal HTN.
- Cocaine MI — beta-blockers contraindicated (unopposed alpha); use benzodiazepines + nitrates.
- Cheese reaction — tyramine + MAO-A inhibitor → hypertensive crisis.
- Anaphylaxis — adrenaline 0.5 mg IM (not subcutaneous).
- Septic shock vasopressor of choice — noradrenaline.
- Asthma maintenance — LABA always with ICS (FDA black box on monotherapy).
- Mirabegron — beta-3 agonist for overactive bladder; alternative to anticholinergics.
- Salmeterol vs formoterol — both LABA; formoterol has faster onset.
- Selegiline — MAO-B at low dose (PD); MAO-A at high dose (caution with tyramine).
- Donepezil + memantine — Alzheimer disease combination.
- Neostigmine reversal of NMB — give with glycopyrrolate to block muscarinic effects.
- Sugammadex — selective relaxant binding agent; reverses rocuronium and vecuronium specifically.
Recent updates and Indian context
- WHO Class I OP ban — India has phased out parathion, methyl parathion, monocrotophos; further restrictions on chlorpyrifos under review.
- Nebivolol — increasingly prescribed in India for HTN due to favourable metabolic profile.
- Carvedilol + bisoprolol + metoprolol succinate — the three "mortality-reducing" beta-blockers in heart failure (mnemonic "Big-CMB").
- Pralidoxime cost barrier — supply gaps in district hospitals; mortality from OP poisoning remains 15 to 25 percent in tertiary Indian series.
- Dexmedetomidine — preferred ICU sedative; less delirium than midazolam; widely available.
- Mirabegron and vibegron — beta-3 agonists added to Indian formularies; alternative to anticholinergics for overactive bladder in elderly.
- Smoking cessation — varenicline + bupropion + NRT under NTCP (National Tobacco Control Programme); MPower MPOWER framework.
Frequently asked questions
What is the difference between direct and indirect cholinergic agonists?
Direct cholinergic agonists bind muscarinic or nicotinic receptors directly — pilocarpine (M, glaucoma), bethanechol (M, urinary retention), methacholine (M, asthma challenge testing), nicotine, varenicline. Indirect cholinergic agonists are acetylcholinesterase inhibitors — they raise endogenous ACh by blocking its breakdown. Examples include neostigmine and pyridostigmine for myasthenia gravis, edrophonium (short-acting; old Tensilon test), donepezil/rivastigmine/galantamine for Alzheimer disease, and the organophosphates (irreversible AChE inhibitors used as pesticides and nerve agents).
How do you manage organophosphate poisoning?
Organophosphate poisoning causes cholinergic crisis from irreversible inhibition of acetylcholinesterase (DUMBBELS muscarinic + nicotinic features). Management — (1) decontaminate clothes/skin, ABC + intubation if respiratory failure; (2) atropine titrated to drying of secretions and clear lungs (start 2 to 4 mg IV, double every 5 minutes until atropinised); (3) pralidoxime (2-PAM) 1 to 2 g IV over 30 minutes within 24 hours, before 'ageing' of the enzyme-OP complex; (4) supportive care + ventilation. India accounts for about one-third of global OP suicide deaths.
Which beta-1 selective and non-selective beta-blockers should I know?
Beta-1 selective ('cardioselective') — atenolol, metoprolol, bisoprolol, esmolol (ultra short-acting IV), nebivolol. Non-selective — propranolol, nadolol, timolol, sotalol. Beta + alpha-1 — carvedilol (heart failure), labetalol (hypertensive emergency, pregnancy). Selectivity is dose-dependent; at high doses cardioselective agents also block beta-2. Nebivolol is unique in having vasodilatory NO-releasing activity. Sotalol has class III antiarrhythmic activity (K+ channel block). Beta-blockers reduce mortality in heart failure, post-MI, and arrhythmias.
What is the mechanism of clonidine and where is it used?
Clonidine is a central alpha-2 adrenergic agonist that activates presynaptic alpha-2 receptors in the rostral ventrolateral medulla, reducing sympathetic outflow and lowering blood pressure, heart rate, and noradrenaline release. Uses include hypertension (especially urgency), opioid and alcohol withdrawal (suppresses sympathetic surge), ADHD, hot flushes, and as an anaesthesia adjunct (sedation + analgesia). Side effects — sedation, dry mouth, bradycardia, and rebound hypertension on abrupt withdrawal (taper required). Dexmedetomidine is a more selective alpha-2 agonist used for ICU sedation.
How is alpha-1 blockade clinically useful?
Alpha-1 antagonists block postsynaptic alpha-1 receptors on vascular smooth muscle (vasodilation), bladder neck and prostate (relaxation). Non-selective alpha (phenoxybenzamine — irreversible, long-acting) is used preoperatively for pheochromocytoma. Selective alpha-1 antagonists are used for benign prostatic hyperplasia (tamsulosin and silodosin are uroselective for alpha-1A on prostate; less postural hypotension than terazosin or doxazosin). Prazosin is used for PTSD nightmares and resistant hypertension. First-dose hypotension is a class effect.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026