Quick Answer
GI physiology is a 2 to 4 question topic per NEET PG paper. Lock these:
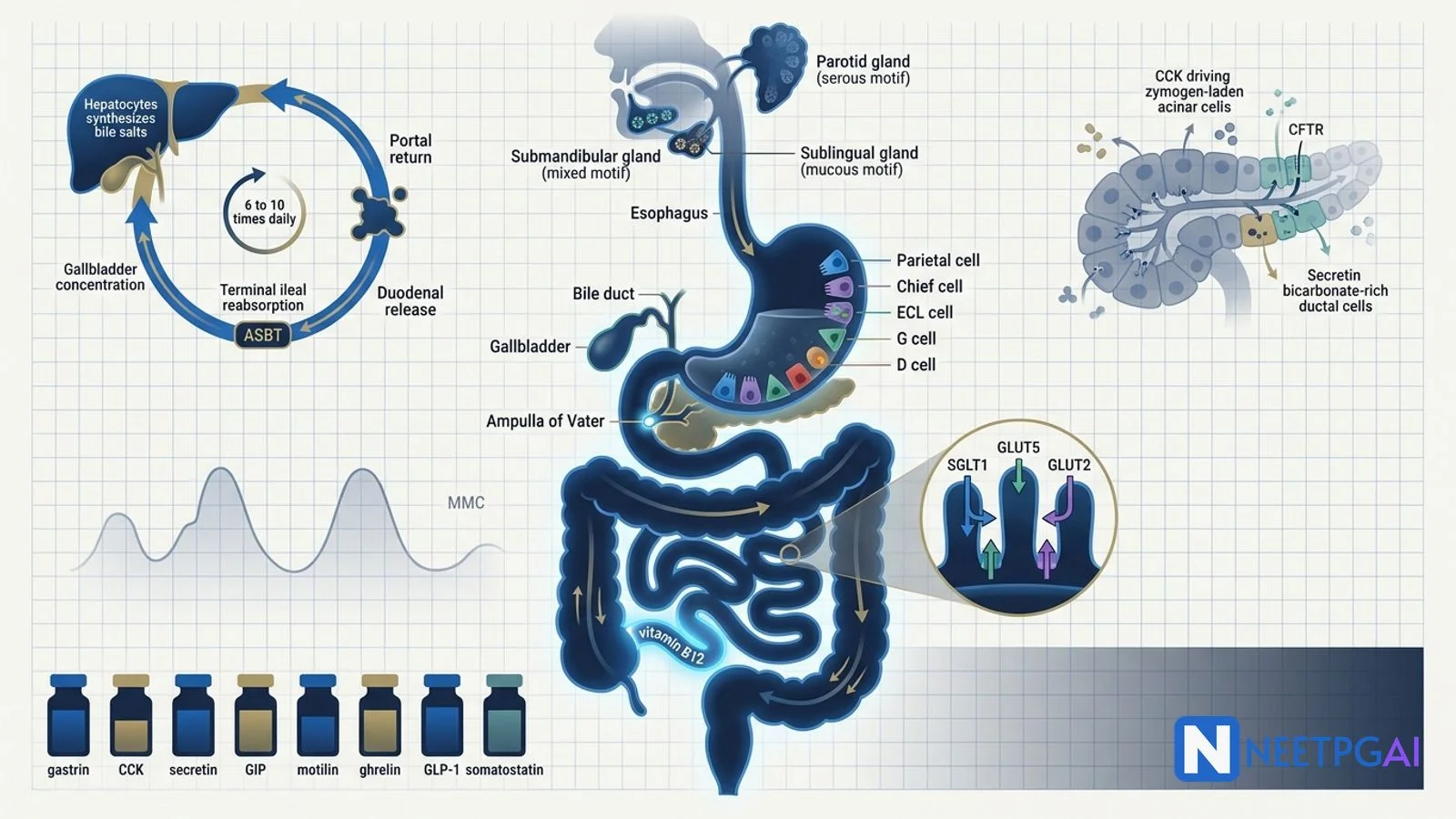
- Parietal cells — HCl (H+/K+ ATPase, omeprazole target) + intrinsic factor.
- Chief cells — pepsinogen. G cells — gastrin. ECL — histamine. D cells — somatostatin.
- Glucose absorption — apical SGLT1, basolateral GLUT2. Fructose — GLUT5 apical.
- Migrating motor complex (MMC) — fasting state, driven by motilin, 90-minute cycle.
- CCK — gallbladder contraction + pancreatic enzyme secretion + Oddi relaxation.
- Secretin — pancreatic and biliary bicarbonate output.
- Bile — enterohepatic recirculation 6 to 10 times daily; terminal ileum reabsorbs salts.
Gastrointestinal physiology is a high-yield topic that overlaps with pharmacology (PPIs, octreotide), biochemistry (lipid digestion, B12 absorption) and medicine (malabsorption syndromes, diarrhoea). The smart move for NEET PG 2026 is to lock the secretion → digestion → absorption → motility sequence, learn the 5 gut-hormone identities cold, and rehearse the classical transporter pairs (SGLT1/GLUT2, GLUT5/GLUT2, NPC1L1 for cholesterol).
This NEETPGAI deep dive walks through salivary, gastric, pancreatic and biliary secretion, macronutrient digestion and absorption, motility patterns (slow waves, MMC, segmentation, peristalsis), and the gut-hormone table. Pair this with the autonomic pharmacology guide for ANS control of GI smooth muscle.
Salivary secretion
Three paired major glands plus minor glands produce 1 to 1.5 L of saliva daily.
| Gland | Type | Innervation | Key enzyme |
|---|
| Parotid | Serous | Glossopharyngeal (CN IX) via otic ganglion | Alpha-amylase (ptyalin) |
| Submandibular | Mixed (serous predominant) | Facial (CN VII) via submandibular ganglion | Amylase + mucin |
| Sublingual | Mucous | Facial (CN VII) via submandibular ganglion | Mucin |
Saliva is hypotonic at low flow (high duct Na+/Cl- reabsorption, K+/HCO3- secretion) and less hypotonic at high flow rates (less time for ductal modification). Functions — lubrication, alpha-amylase starch digestion, lingual lipase (limited fat digestion, important in neonates), antibacterial (lysozyme, lactoferrin, IgA), bicarbonate buffering of refluxed acid.
Parasympathetic stimulation produces a copious, watery, enzyme-rich saliva (atropine causes xerostomia). Sympathetic stimulation produces a small, viscous saliva.
Gastric secretion
The stomach produces 2 to 3 L/day of secretions. Cell types in the gastric body and antrum:
| Cell | Location | Secretion | Function |
|---|
| Parietal (oxyntic) | Body | HCl + intrinsic factor | Acid digestion, B12 absorption |
| Chief (peptic) | Body | Pepsinogen | Protein digestion (after activation at pH < 3) |
| ECL (enterochromaffin-like) | Body | Histamine | Paracrine acid stimulation |
| G cells | Antrum | Gastrin | Endocrine acid stimulation |
| D cells | Body + antrum | Somatostatin | Inhibits gastrin and HCl |
| Mucous neck | Body | Mucus + HCO3- | Mucosal protection |
HCl secretion mechanism
Parietal cells secrete HCl via the H+/K+ ATPase on the apical (canalicular) membrane. This is the molecular target of PPIs (omeprazole, pantoprazole — irreversible covalent inhibitors). The basolateral Cl-/HCO3- exchanger generates the "alkaline tide" in venous blood after a meal.
Three phases of acid secretion
- Cephalic phase (~30%) — sight/smell/taste/chewing → vagal stimulation → ACh on M3 receptors of parietal cells + GRP on G cells.
- Gastric phase (~60%) — distension + peptides → vagovagal reflex + direct G-cell activation by aromatic amino acids → gastrin.
- Intestinal phase (~10%) — duodenal chyme triggers secretin, CCK, GIP — mostly inhibitory to the stomach.
Three direct stimulants of HCl (the "three-arm" model)
- Gastrin (G cells) → CCK-B receptor on parietal cell → Gq → Ca2+.
- ACh (vagus) → M3 receptor → Gq → Ca2+.
- Histamine (ECL) → H2 receptor → Gs → cAMP. (H2 blockers like ranitidine target this.)
Somatostatin inhibits all three via the D cell — the dominant brake. Omeprazole works downstream of all three at the H+/K+ ATPase, hence its potency.
Pancreatic secretion
Two functional compartments — acinar (enzyme) and ductal (bicarbonate). Total output 1.5 L/day, isotonic with plasma.
- Acinar cells secrete digestive enzymes — trypsinogen, chymotrypsinogen, procarboxypeptidase, pancreatic lipase, colipase, phospholipase A2, alpha-amylase, ribonuclease, deoxyribonuclease. Stimulated mainly by CCK via vagal cholinergic pathway.
- Ductal cells secrete a watery NaHCO3-rich juice via apical CFTR (cystic fibrosis target). Stimulated mainly by secretin in response to acidic chyme (pH < 4.5) entering the duodenum.
Trypsinogen is converted to trypsin by enterokinase on the duodenal brush border; trypsin then activates other proenzymes (cascade activation). Premature intrapancreatic trypsin activation causes acute pancreatitis (gallstones, alcohol, hypertriglyceridaemia — most common Indian aetiologies).
Bile and enterohepatic circulation
Hepatocytes synthesise primary bile acids — cholic and chenodeoxycholic acid — from cholesterol via 7α-hydroxylase (the rate-limiting step). Conjugation with glycine or taurine makes them more water-soluble. Gut bacteria convert primary to secondary bile acids — deoxycholic and lithocholic acid.
Bile components — bile salts, phospholipids (lecithin), cholesterol, bilirubin (conjugated), water, electrolytes. Bile is concentrated 5- to 20-fold in the gallbladder by NaCl-driven water reabsorption.
Enterohepatic circulation — 95 percent of bile salts are actively reabsorbed in the terminal ileum via ASBT (apical sodium-dependent bile acid transporter), return to the liver via portal blood, and are re-secreted. Total bile salt pool 2 to 4 g recirculates 6 to 10 times daily. Terminal ileal resection or Crohn disease causes bile salt malabsorption, fat-soluble vitamin deficiency, and gallstones.
Digestion of macronutrients
Carbohydrates
Salivary and pancreatic alpha-amylases cleave starch (alpha-1,4 bonds) to maltose, maltotriose, and alpha-limit dextrins. Brush border enzymes complete digestion to monosaccharides — lactase (lactose → glucose + galactose), sucrase (sucrose → glucose + fructose), maltase and isomaltase. Lactase deficiency (very high prevalence in adult Indians) causes osmotic diarrhoea and bloating.
Proteins
Pepsin (gastric, pH 1.5 to 3) begins protein digestion. Trypsin, chymotrypsin, elastase, carboxypeptidases (pancreatic) and brush border aminopeptidases complete it. Amino acids and di-/tripeptides are absorbed via specific apical transporters (PepT1 for di-/tripeptides).
Fats
Pancreatic lipase (with colipase) hydrolyses triglycerides to 2-monoglyceride and free fatty acids. Bile salts form mixed micelles delivering products to the apical enterocyte membrane. Inside the enterocyte, triglycerides are re-synthesised, packaged with apoB-48 into chylomicrons, and exit basolaterally into lymphatics (lacteals → thoracic duct → systemic circulation).
Absorption — key transporters
| Nutrient | Apical transporter | Basolateral exit |
|---|
| Glucose, galactose | SGLT1 (Na+-coupled, secondary active) | GLUT2 (facilitated) |
| Fructose | GLUT5 (facilitated) | GLUT2 (facilitated) |
| Cholesterol | NPC1L1 (ezetimibe target) | Chylomicron via ABCG5/G8 efflux back |
| Iron (haem) | HCP1 | Ferroportin (hepcidin-regulated) |
| Iron (non-haem) | DMT1 (after Fe3+ → Fe2+ by Dcytb) | Ferroportin |
| Vitamin B12 | IF-B12 complex via cubilin in terminal ileum | Transcobalamin II |
| Bile salts | ASBT (terminal ileum) | OSTα/β |
| Calcium | TRPV6 (active, vitamin D regulated) | PMCA + NCX |
GI motility
Smooth muscle of the GI tract is electrically coupled by gap junctions and shows resting slow waves generated by the interstitial cells of Cajal (ICC — the pacemakers). Slow waves alone do not cause contraction; they must reach threshold for a spike potential (action potential) which triggers contraction.
| Region | Slow wave frequency |
|---|
| Stomach | 3/min |
| Duodenum | 12/min |
| Ileum | 8/min |
| Colon | 3 to 12/min (variable) |
Motility patterns
- Migrating motor complex (MMC) — fasting state housekeeping waves, driven by motilin from duodenal M cells; abolished by eating. Erythromycin is a motilin agonist (used for gastroparesis).
- Segmentation — non-propulsive mixing contractions of the small intestine.
- Peristalsis — coordinated propulsive waves (proximal contraction + distal relaxation); the law of the gut.
- Mass movement — strong propagating colonic contractions 1 to 3 times daily, often after meals (gastrocolic reflex).
Sphincters and reflexes
- Lower oesophageal sphincter (LES) — relaxed by VIP and NO from inhibitory neurons; tonically contracted to prevent reflux. Achalasia is failure of LES relaxation due to loss of inhibitory neurons.
- Gastrocolic reflex — distension of stomach causes increased colonic motility (mediated by gastrin and ANS).
- Defecation reflex — distension of rectum → sacral parasympathetic (S2-S4) → internal anal sphincter relaxation + external (voluntary) control.
Gut hormones at a glance
| Hormone | Cell | Stimulus | Main action |
|---|
| Gastrin | G (antrum) | Distension, peptides, vagus | HCl + parietal cell growth |
| CCK | I (duodenum, jejunum) | Fatty acids, amino acids | Gallbladder contraction, pancreatic enzymes, Oddi relaxation |
| Secretin | S (duodenum) | Acidic chyme (pH < 4.5) | Pancreatic/biliary HCO3-; inhibits gastrin |
| GIP | K (duodenum, jejunum) | Glucose, fat | Insulin release (incretin); inhibits HCl |
| Motilin | M (duodenum) | Fasting | MMC initiation |
| Ghrelin | P/D1 (stomach) | Fasting | Hunger; GH release |
| VIP | Pancreatic islets, gut neurons | — | Smooth muscle relaxation, water/electrolyte secretion |
| Somatostatin | D cells | Acid, multiple | Inhibits all GI hormones, "off-switch" |
| GLP-1 | L (ileum, colon) | Carbs, fat | Insulin (incretin), satiety, slowed gastric emptying |
GLP-1 underlies the semaglutide / liraglutide / tirzepatide mechanism — the GLP-1 receptor agonists revolutionising T2DM and obesity therapeutics.
NEET PG MCQ traps
- HCl pump — H+/K+ ATPase on parietal cell apical membrane; PPI target.
- Pernicious anaemia — autoimmune parietal cell destruction → no IF → B12 malabsorption + megaloblastic anaemia.
- Zollinger-Ellison syndrome — gastrinoma → recurrent peptic ulcers, diarrhoea; secretin paradoxically increases gastrin (diagnostic test).
- SGLT1 — apical glucose/galactose; GLUT5 — apical fructose; GLUT2 — basolateral exit for all three.
- NPC1L1 — apical cholesterol uptake; ezetimibe target.
- Vitamin B12 absorption — terminal ileum via IF-B12 complex and cubilin receptor. Crohn disease and ileal resection cause deficiency.
- Enterokinase — duodenal brush border; activates trypsinogen → trypsin (master switch for pancreatic enzymes).
- Pancreatic bicarbonate — secretin-driven via CFTR; abolished in cystic fibrosis.
- MMC driver — motilin; abolished by eating; erythromycin is motilin agonist.
- Slow wave frequency — stomach 3/min, duodenum 12/min, ileum 8/min.
- Achalasia — loss of inhibitory neurons in LES; failure of relaxation; bird-beak on barium.
- CCK — fatty acid stimulus → gallbladder contraction + pancreatic enzymes + Oddi relaxation.
- Secretin — acid stimulus → bicarbonate (not HCl).
- GIP and GLP-1 — incretins, augment glucose-stimulated insulin secretion.
- Ghrelin — only hunger-promoting gut hormone; rises in fasting.
- Lactase deficiency — adult Indian prevalence high; osmotic diarrhoea + bloating after dairy.
- Bile salt reabsorption — terminal ileum (ASBT). Resection or Crohn → bile salt malabsorption + steatorrhoea.
- Chylomicrons — exit enterocyte into lacteals (lymphatics), not portal vein.
Recent updates and Indian context
- Helicobacter pylori — prevalence in Indian adults 60 to 80 percent; major cause of peptic ulcer and gastric adenocarcinoma. Triple therapy (PPI + clarithromycin + amoxicillin) still first-line.
- Lactose intolerance — over 70 percent prevalence in adult Indians from south India; hydrogen breath test for diagnosis.
- Tropical sprue — endemic in south India; small bowel villous atrophy + folate/B12 deficiency; treat with tetracycline + folate.
- GLP-1 agonists — semaglutide and tirzepatide rapidly entering Indian endocrine practice for T2DM and obesity; mechanism rooted in gut-hormone physiology.
- PPI overuse — long-term acid suppression linked to B12 deficiency, hypomagnesaemia, C. difficile, and CKD; deprescribing is now an exam-relevant theme.
Frequently asked questions
Which cells secrete HCl and what is the role of intrinsic factor?
Parietal (oxyntic) cells in the gastric body secrete both hydrochloric acid (HCl) and intrinsic factor (IF). HCl is secreted via the H+/K+ ATPase proton pump on the apical membrane (the target of omeprazole). Intrinsic factor is a glycoprotein that binds vitamin B12 in the duodenum and is essential for its absorption in the terminal ileum. Autoimmune destruction of parietal cells (pernicious anaemia) abolishes both functions, causing megaloblastic anaemia and achlorhydria.
What is the migrating motor complex (MMC) and when does it occur?
The migrating motor complex is a cyclical pattern of GI motility that occurs during the fasting state (interdigestive period). It has four phases lasting around 90 to 120 minutes total — phase I quiescence, phase II irregular contractions, phase III strong propagating contractions sweeping from stomach to terminal ileum, and phase IV transition. The MMC is driven primarily by motilin from M cells of the duodenum. Its housekeeping function clears residual contents and bacteria; eating immediately abolishes the MMC.
How is glucose absorbed in the small intestine?
Glucose absorption is a two-step transcellular process. At the apical (luminal) membrane, glucose enters enterocytes via SGLT1 (sodium-glucose linked transporter 1) — secondary active transport coupled to the Na+ gradient maintained by the basolateral Na+/K+ ATPase. At the basolateral membrane, glucose exits into the portal blood via GLUT2 (facilitated diffusion down its concentration gradient). Galactose uses the same SGLT1/GLUT2 pair. Fructose uses GLUT5 apically (facilitated diffusion) and GLUT2 basolaterally.
What are the three phases of gastric acid secretion?
Gastric acid secretion has cephalic, gastric, and intestinal phases. The cephalic phase (around 30 percent) is triggered by sight, smell, taste, and chewing — mediated via the vagus nerve releasing acetylcholine onto parietal cells and gastrin-releasing peptide onto G cells. The gastric phase (around 60 percent) is triggered by gastric distension and peptides activating G cells to release gastrin. The intestinal phase (around 10 percent) is triggered by chyme in the duodenum and is dominantly inhibitory via secretin, CCK, and GIP, which down-regulate gastric acid.
What is the role of CCK in fat digestion?
Cholecystokinin (CCK) is released from I cells of the duodenum and jejunum in response to luminal fatty acids and amino acids. Its three classical actions are gallbladder contraction (delivers bile salts for fat emulsification and micelle formation), pancreatic acinar enzyme secretion (lipase, amylase, trypsinogen, chymotrypsinogen), and relaxation of the sphincter of Oddi. CCK also slows gastric emptying and promotes satiety. CCK acts via CCK-A receptors on the gallbladder and pancreas.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026