image mcq
radiology
orthopedics
bone tumor
osteosarcoma
ewing sarcoma
paget disease
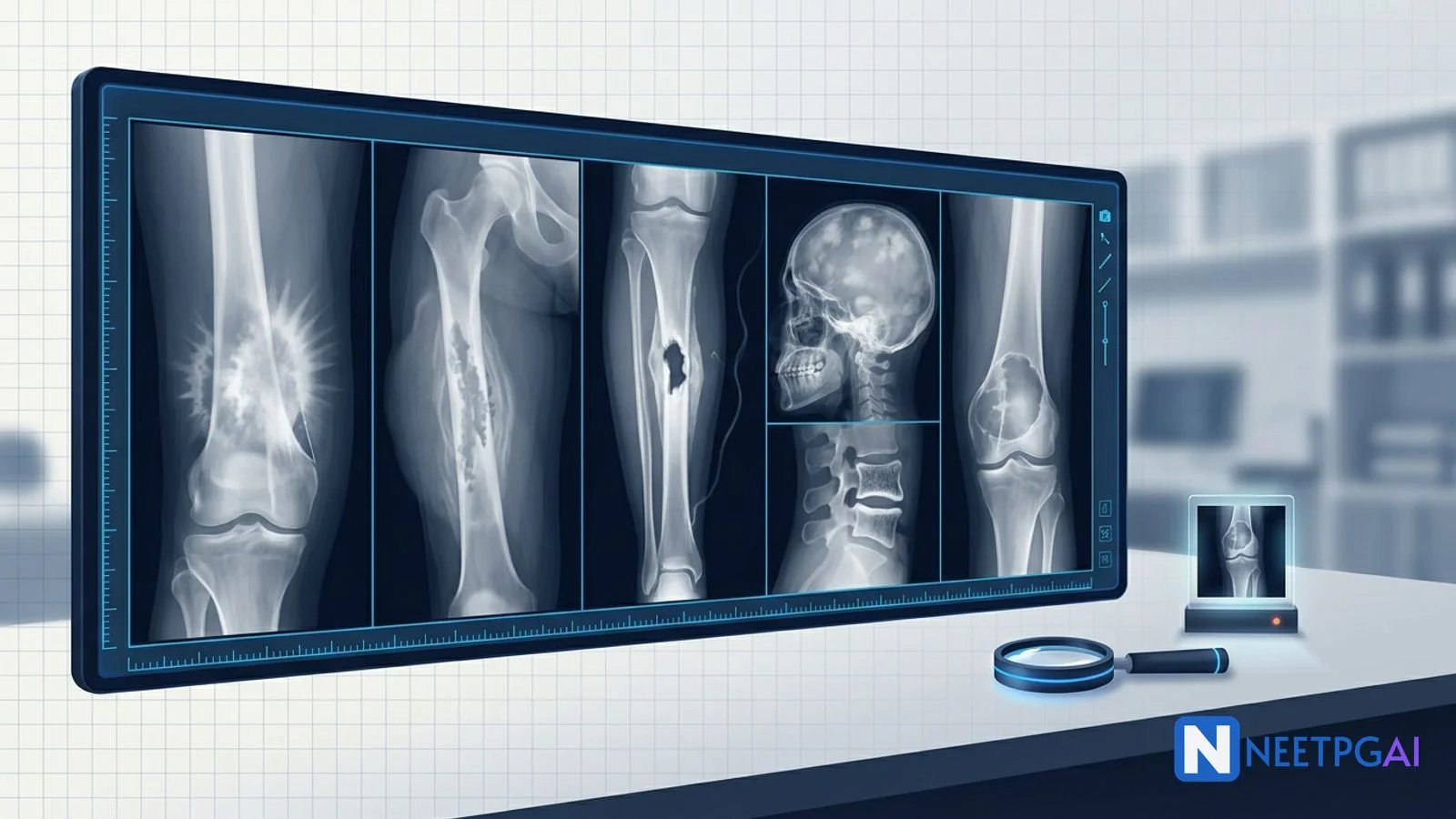
5 high-yield bone X-ray image MCQs for NEET PG: osteosarcoma sunburst, Ewing onion-skin, chronic osteomyelitis sequestrum, Paget cotton wool, GCT soap bubble — with teaching pearls.
Version 1.0 — Published May 2026
Bone X-ray pathology contributes 3-5 questions per NEET PG paper across orthopedics, radiology, and pathology. Five patterns recur reliably:
Combine the age + location + margin + periosteal reaction + matrix rule and almost every NEET PG bone X-ray collapses to a 30-second answer.
Bone radiographs sit at the intersection of orthopaedics, radiology, pathology, and oncology. NEET PG and FMGE feature bone X-ray images in 3-5 questions per paper, often using a single iconic image to test the entire diagnostic chain — pattern recognition, differential, biopsy approach, and management.
The patterns are highly stereotyped and well-described in textbooks. Drilling 5 patterns plus 5-10 PYQ bone X-ray images daily for 2 weeks moves accuracy from 40 to 80 percent on this domain.
Six features evaluated on every bone lesion X-ray:
| Feature | What to look for | Implication |
|---|---|---|
| Patient age | Under 5, 5-30, 30-40, over 40 | Different differential at each age band |
| Location in bone | Epiphysis, metaphysis, diaphysis | Each location has its own short list |
| Margin / zone of transition | Narrow sclerotic = benign; wide moth-eaten/permeative = aggressive | Aggressive ≈ malignant or infection |
| Periosteal reaction | Solid/buttress (benign); onion-skin/sunburst/Codman triangle (aggressive) | Driven by speed of growth |
| Matrix mineralisation | Chondroid (rings/arcs, popcorn); osteoid (cloud); fibrous (ground-glass) | Identifies tissue of origin |
| Soft-tissue extension |
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeMaster GI secretions, digestion, absorption transporters, motility patterns, and gut hormones with high-yield NEET PG 2026 traps and India-context examples.
Master labor stages, Friedman vs Zhang curves, WHO partograph, AMTSL, episiotomy and India JSY/LaQshya policies for NEET PG 2026 OBG MCQs.
5 anterior segment ophthalmology image MCQs for NEET PG: hypopyon and Behcet, Kayser-Fleischer ring in Wilson, Brushfield spots in Down, corneal arcus, and pterygium vs pinguecula.
| Soft-tissue mass with cortical break |
| Aggressive lesion |
| Age | Common entities |
|---|---|
| Under 5 | Metastatic neuroblastoma, Ewing sarcoma, eosinophilic granuloma, leukemia, infection |
| 5-30 | Osteosarcoma, Ewing sarcoma, osteoblastoma, osteoid osteoma, simple bone cyst, ABC, fibrous dysplasia |
| 30-40 | GCT, chondrosarcoma, fibrous dysplasia, enchondroma |
| Over 40 | Metastasis, multiple myeloma, lymphoma, chondrosarcoma, Paget disease |
| Location | Lesions |
|---|---|
| Epiphysis | GCT (after physeal closure), chondroblastoma (before closure), clear cell chondrosarcoma, infection |
| Metaphysis | Osteosarcoma, non-ossifying fibroma, simple bone cyst, ABC, osteomyelitis |
| Diaphysis | Ewing sarcoma, fibrous dysplasia, adamantinoma, osteoid osteoma, lymphoma |
Image description: [Plain AP and lateral X-ray of the right distal femur in a 14-year-old. There is an aggressive metaphyseal lesion with mixed lytic and sclerotic ('cloud-like' osteoid matrix) appearance occupying the metaphysis. Wide zone of transition. Cortical breakthrough on the lateral aspect with a soft-tissue mass. Sunburst (sunray) periosteal reaction with spicules of new bone radiating perpendicular to the cortex. Codman triangle at the proximal margin where the periosteum is elevated and ossified at the edge. The growth plate appears intact (lesion does not cross into epiphysis). Skeletal maturity consistent with age — physis still open.]
Clinical vignette: A 14-year-old schoolboy presents with progressive pain and swelling around the right knee for 6 weeks. The pain is worse at night, partially relieved by NSAIDs but never fully. He noticed a hard tender lump above the knee. No fever. No weight loss. No history of trauma. On examination there is a firm, warm, tender swelling at the distal femur with limited knee flexion. Investigations: serum alkaline phosphatase 580 U/L (normal up to 130 in adults; raised even for adolescent reference range), serum LDH 540 U/L, normal CBC and ESR.
Options:
Correct answer: (a) Osteosarcoma
Reasoning: Adolescent age (peak 10-20), distal femur metaphysis (the commonest site, around the knee where 60 percent of osteosarcomas occur), aggressive lytic-sclerotic lesion with cloud-like osteoid matrix, sunburst periosteal reaction with spicules perpendicular to the cortex, Codman triangle, soft-tissue mass, and raised serum alkaline phosphatase and LDH are textbook for conventional osteosarcoma.
Ewing sarcoma is also bimodal in adolescents but typically occupies the diaphysis (not metaphysis), produces onion-skin lamellated periosteal reaction rather than sunburst, and does not produce osteoid matrix. Acute osteomyelitis can mimic but typically has higher inflammatory markers (raised CRP/ESR), fever, and a more permeative pattern; ALP and LDH are not raised. Aneurysmal bone cyst is purely lytic without osteoid matrix and produces an expansile blown-out appearance, not aggressive periosteal reaction.
Teaching pearl: Osteosarcoma triad on X-ray = sunburst periosteal reaction + Codman triangle + cloud-like osteoid matrix. Plus age (peak 10-20), location (around the knee — distal femur > proximal tibia > proximal humerus), and biochemistry (raised ALP and LDH).
Workup after imaging:
Treatment: Neoadjuvant chemotherapy (MAP regimen — methotrexate, doxorubicin, cisplatin) → limb-sparing wide local excision (or amputation if neurovascular bundle involvement) → adjuvant chemotherapy. Five-year survival for non-metastatic disease 60-70 percent; metastatic at presentation drops to 20-30 percent.
Subtypes worth knowing: parosteal (low-grade, posterior distal femur, surface lesion, better prognosis), periosteal (intermediate-grade, diaphyseal, surface), telangiectatic (lytic, fluid-fluid levels — can mimic ABC), and small-cell osteosarcoma (mimics Ewing).
Predisposing conditions: Paget disease (1 percent transformation risk), prior radiation, hereditary retinoblastoma (RB1 mutation), Li-Fraumeni syndrome (TP53 mutation), Rothmund-Thomson syndrome.
Image description: [Plain AP X-ray of the left mid-femur in a 12-year-old. There is a permeative lytic lesion in the diaphysis of the femur with ill-defined margins and a wide zone of transition. Multilayered lamellated 'onion-skin' periosteal reaction is the dominant feature, with several concentric layers of new periosteal bone parallel to the cortex. There is a large soft-tissue mass extending beyond the cortex into the surrounding muscle, larger than the bony component itself. No osteoid or chondroid matrix. The growth plate is open and intact.]
Clinical vignette: A 12-year-old boy presents with 3 weeks of progressive left thigh pain and a low-grade fever (37.8 C). On examination there is a tender swelling at the mid-thigh with overlying warmth. Labs: WBC 13,000 with mild left shift, ESR 78 mm/hr, CRP 64 mg/L, LDH 720 U/L, normal ALP for age, normal calcium and phosphate. Bone biopsy shows sheets of small round blue cells with scant cytoplasm; immunohistochemistry positive for CD99 (membranous), FLI1, NKX2.2; cytogenetics show t(11;22)(q24;q12) producing EWSR1-FLI1 fusion.
Options:
Correct answer: (b) Ewing sarcoma
Reasoning: Age 12, diaphyseal location of femur, permeative lytic lesion, classic onion-skin lamellated periosteal reaction, large soft-tissue component (often disproportionate to the bony lesion), low-grade fever and raised inflammatory markers (often confused with infection), raised LDH, and confirmatory histology with CD99 positivity and t(11;22) EWSR1-FLI1 fusion are textbook Ewing sarcoma.
Acute osteomyelitis is the closest mimic — fever, raised inflammatory markers, periosteal reaction. The discriminator is biopsy (Ewing sarcoma cells vs pus and bacteria), the cytogenetic translocation (Ewing-specific), and the larger soft-tissue mass in Ewing relative to the bony lesion. Osteosarcoma occurs in metaphysis, has osteoid matrix and sunburst rather than onion-skin. Eosinophilic granuloma can produce permeative lesions and onion-skin periosteum but typically has a more focal lytic lesion ('floating teeth' in mandible, 'vertebra plana') and biopsy shows Langerhans cells with CD1a and S100 positivity.
Teaching pearl: Ewing sarcoma key features — child/adolescent, diaphyseal, onion-skin periosteal reaction, large soft-tissue component, CD99-positive small round blue cell tumor, t(11;22) EWSR1-FLI1 fusion. The fever and raised inflammatory markers are the classic 'osteomyelitis mimic' trap.
Workup after imaging:
Treatment: Neoadjuvant chemotherapy (vincristine, doxorubicin, cyclophosphamide alternating with ifosfamide and etoposide — VDC/IE) → local control (surgery and/or radiation; Ewing is radiosensitive unlike osteosarcoma) → adjuvant chemotherapy. Five-year survival for localised disease 70-80 percent; metastatic 20-30 percent.
Differentiator vs osteosarcoma (NEET PG favourite):
| Feature | Osteosarcoma | Ewing sarcoma |
|---|---|---|
| Age peak | 10-20 | 5-15 |
| Location | Metaphysis (around knee) | Diaphysis (femur, pelvis) |
| Matrix | Osteoid (cloud-like) | None |
| Periosteal reaction | Sunburst, Codman triangle | Onion-skin, Codman triangle |
| Histology | Spindle cells producing osteoid | Small round blue cells, CD99+ |
| Cytogenetics | TP53, RB1 (often) | t(11;22) EWSR1-FLI1 |
| Radiosensitive | No | Yes |
| Biochemistry | Raised ALP and LDH | Raised LDH; mild inflammatory markers |
Image description: [Plain AP X-ray of the right tibia in a 28-year-old man. There is a mixed lytic-sclerotic lesion involving the mid-shaft of the tibia. A central sequestrum appears as a denser sclerotic fragment of dead bone surrounded by a lucent zone, separated from the surrounding bone. A surrounding new periosteal sleeve of thickened bone (involucrum) encases the sequestrum. There is an opening (cloaca) in the involucrum on the anteromedial cortex through which a sinus tract communicates with the soft tissues. Cortical thickening is present. Soft-tissue swelling overlying the cloaca with a small subcutaneous lucent track to the skin surface.]
Clinical vignette: A 28-year-old labourer presents with a chronic discharging sinus over the right tibia of 14 months' duration. He sustained an open tibial fracture 18 months ago in a road traffic accident, treated initially with debridement and intramedullary nailing. He has had multiple episodes of sinus discharge with intermittent pus and bone fragments, partial closure with antibiotics, and recurrence. Currently afebrile, sinus actively discharging mucopurulent fluid. Examination: cortical thickening on palpation, sinus opening with surrounding granulation tissue. Labs: ESR 58 mm/hr, CRP 32 mg/L, WBC normal, hemoglobin 11.4. Wound swab grows Staphylococcus aureus sensitive to cloxacillin. MRI shows the sequestrum hypointense on all sequences, surrounding marrow edema and a Brodie-like cavity.
Options:
Correct answer: (a) Chronic osteomyelitis with sequestrum, involucrum, and cloaca
Reasoning: Open fracture history, chronic discharging sinus, mixed lytic-sclerotic tibial lesion with the classic triad of sequestrum (dead bone) + involucrum (new periosteal sleeve) + cloaca (drainage opening), and growth of S. aureus from the discharge is textbook chronic osteomyelitis following open trauma.
Osteoid osteoma is a small (under 1.5 cm), well-defined, lucent nidus with surrounding sclerosis, often subperiosteal, classically causing nocturnal pain relieved by NSAIDs — no sequestrum, no sinus. Tuberculous osteomyelitis can produce chronic sinus and cold abscess but classically affects vertebra (Pott's), is paucibacillary on smear, has an indolent course with weight loss, and shows discrete vertebral collapse with paraspinal abscess on imaging. Stress fracture is a discrete fracture line with callus, no sequestrum.
Teaching pearl: Chronic osteomyelitis triad — sequestrum (dead bone separated from healthy bone, hyperdense on X-ray) + involucrum (new periosteal bone surrounding the sequestrum, often thickening the cortex) + cloaca (opening in the involucrum through which pus and necrotic bone drain). A sinus tract to skin surface is the clinical correlate. Brodie's abscess is a localised intramedullary subacute osteomyelitis with a sclerotic rim — most often tibial metaphysis.
Etiology:
Workup:
Treatment:
Failed therapy may require amputation, particularly for diabetic foot osteomyelitis with extensive necrosis.
Cierny-Mader staging of chronic osteomyelitis combines anatomical extent (medullary, superficial, localised, diffuse) and host status (A — normal; B — compromised local or systemic; C — therapy worse than disease) — guides surgical aggressiveness.
Image description: [Lateral skull X-ray and AP X-ray of the tibia in a 64-year-old. Skull shows multiple ill-defined sclerotic patches with a 'cotton-wool' appearance against the diploic space; calvarial thickening is generalised; the inner and outer tables are blurred. The pituitary fossa appears slightly enlarged. Tibial AP shows an enlarged, thickened, and bowed tibia with coarsened trabecular pattern, cortical thickening, and a 'flame' or 'V-shaped' lytic advancing front in one segment of the bone — the lytic phase merging into mixed phase. A spine X-ray inset shows a vertebra with thickened cortex around the body producing a 'picture-frame' appearance.]
Clinical vignette: A 64-year-old retired sugarcane farmer presents with progressive frontal headaches, gradual bilateral hearing loss over 2 years, hat-size increase ('my caps don't fit any more'), and increasing bowing of both legs. Cardiac examination reveals mild tachycardia (94/min) without murmur. Investigations: serum alkaline phosphatase 1,420 U/L (markedly raised), serum calcium 9.4 mg/dL (normal), serum phosphate 3.5 mg/dL (normal), urinary hydroxyproline raised, urine deoxypyridinoline raised. Audiogram shows bilateral mixed sensorineural-conductive hearing loss. ECG shows sinus rhythm, mild left ventricular hypertrophy.
Options:
Correct answer: (a) Paget disease of bone
Reasoning: Older adult with raised serum ALP in isolation (normal calcium, phosphate, and other LFT components), cotton-wool skull appearance, bowed and thickened tibia, picture-frame vertebra, hearing loss (CN VIII compression at the skull base), and headache is textbook Paget disease of bone.
Multiple myeloma produces multiple punched-out lytic lesions ('pepper-pot skull' rather than cotton-wool), hypercalcemia, anemia, renal failure, monoclonal protein on SPEP/UPEP — different biochemical and imaging picture. Osteopetrosis ('marble bone disease') is a generalised osteosclerosis with a 'bone-in-bone' appearance, not patchy sclerosis with bowing; presents in childhood usually with marrow failure. Renal osteodystrophy in CKD shows osteomalacia + secondary hyperparathyroidism + osteosclerosis (rugger-jersey spine), with abnormal calcium-phosphate-PTH biochemistry. Fibrous dysplasia produces a ground-glass matrix in young patients, with shepherd's-crook deformity of the femur, but not cotton-wool skull; McCune-Albright if café-au-lait macules and endocrinopathy.
Teaching pearl: Paget disease iconic findings:
Three radiographic phases:
Pathology: disorganised increase in bone turnover with both excessive osteoclastic resorption and excessive disordered osteoblastic deposition; thought to involve a paramyxovirus-like infection of osteoclasts in genetically predisposed individuals (SQSTM1 mutations).
Complications:
Management:
Image description: [Plain AP and lateral X-ray of the right knee in a 26-year-old woman. There is a well-defined, eccentric, expansile lytic lesion in the epiphysis and metaphysis of the distal femur, extending up to the subchondral bone. The lesion has a classic 'soap-bubble' appearance with internal trabeculations. The margin is non-sclerotic and well-defined (narrow zone of transition without a sclerotic rim). The cortex is thinned and minimally expanded, with a subtle cortical breakthrough on one side without a definite soft-tissue mass. No periosteal reaction. No matrix mineralisation. The growth plate is closed (skeletally mature).]
Clinical vignette: A 26-year-old IT professional presents with 5 months of progressive right knee pain, worse with activity, mild swelling, and intermittent stiffness. No fever, no weight loss, no constitutional symptoms. On examination there is a firm tender mass at the distal femur with mild knee effusion. Plain X-rays show the eccentric epiphyseal-metaphyseal lesion described. CT confirms the lytic eccentric lesion, no matrix, cortical thinning. MRI shows a heterogeneous lesion with both solid and cystic components, fluid-fluid levels in some areas. Biopsy shows multinucleated giant cells admixed with mononuclear stromal cells.
Options:
Correct answer: (a) Giant cell tumor of bone (osteoclastoma)
Reasoning: Skeletally mature adult (age 20-40), eccentric epiphyseal lesion extending to subchondral bone, expansile lytic 'soap-bubble' appearance, narrow zone of transition without a sclerotic rim, location around the knee (distal femur or proximal tibia), and biopsy showing multinucleated osteoclast-like giant cells in a stroma of mononuclear cells is textbook giant cell tumor of bone (GCT, osteoclastoma).
ABC also produces an eccentric expansile lytic lesion with fluid-fluid levels but is typically metaphyseal in skeletally immature patients; it lacks the solid component on MRI that GCT shows. Chondroblastoma is also epiphyseal but typically in skeletally immature patients (open physis) and shows a chondroid (rings and arcs, popcorn) matrix; biopsy shows chondroblasts with eosinophilic cytoplasm and 'chicken-wire' calcification. Brown tumor of hyperparathyroidism produces multiple lytic lesions with raised PTH and abnormal calcium-phosphate biochemistry; biopsy can mimic GCT histologically (giant cells in fibrous stroma) — discriminate by biochemistry.
Teaching pearl: GCT classic features — age 20-40 (skeletally mature), epiphyseal extending to subchondral, eccentric, expansile, soap-bubble lytic, narrow zone of transition without sclerotic rim, no matrix, no periosteal reaction. Most common sites: distal femur > proximal tibia (around the knee, ~50 percent) > distal radius (~10 percent) > sacrum.
Behaviour and grading: GCT is locally aggressive with high recurrence rate (20-50 percent after curettage). Approximately 1-3 percent metastasise to lung (benign metastases — histologically identical, usually indolent). Roughly 1-5 percent undergo malignant transformation, particularly after radiotherapy.
Campanacci radiographic grading:
Treatment:
Differential of 'giant cell-rich' bone lesions on biopsy (a NEET PG favourite):
Always correlate biopsy with imaging and clinical context — pure histology can be misleading.
Pitfall 1: Confusing osteosarcoma and Ewing sarcoma. Both occur in adolescents but osteosarcoma is metaphyseal with sunburst + osteoid matrix, while Ewing is diaphyseal with onion-skin and no matrix. The histology and cytogenetics seal the diagnosis.
Pitfall 2: Mistaking Ewing sarcoma for osteomyelitis. Both have fever, raised inflammatory markers, periosteal reaction, and bone destruction. The discriminator is biopsy. Always biopsy a 'persistent osteomyelitis' that doesn't respond to antibiotics.
Pitfall 3: Calling every multinucleated giant cell histology 'GCT'. Brown tumor of hyperparathyroidism, ABC, chondroblastoma, and giant-cell reparative granuloma all share giant cells. Check serum calcium, phosphate, and PTH in any 'GCT' — particularly multifocal GCT-like lesions.
Pitfall 4: Missing osteoid osteoma in nocturnal bone pain. Small (<1.5 cm) lucent nidus surrounded by sclerosis, classic nocturnal pain relieved by aspirin/NSAIDs (prostaglandin-mediated). CT is the imaging gold standard — radiofrequency ablation is the treatment of choice.
Pitfall 5: Ivory vertebra has 4 main differentials. Paget, metastasis (osteoblastic — prostate, breast), lymphoma, and (less commonly) chronic osteomyelitis. Don't anchor on Paget without checking for primary malignancy.
Pitfall 6: Cotton-wool skull is not 'pepper-pot skull'. Cotton-wool = ill-defined SCLEROTIC patches in Paget. Pepper-pot (or 'salt-and-pepper') = small punched-out LYTIC lesions in multiple myeloma or hyperparathyroidism. Direction of contrast is opposite.
Pitfall 7: Forgetting age in GCT. GCT requires a CLOSED growth plate. Epiphyseal lesion in a child with open physis is more likely chondroblastoma. Epiphyseal lesion after closure is GCT.
Six recurring patterns. Recognise the pattern and the question collapses.
Pattern 1 — The osteosarcoma question: Adolescent with painful swelling around the knee, X-ray showing sunburst + Codman triangle + cloud-like matrix. Diagnosis? Osteosarcoma. Site of metastasis? Lung first. Treatment? Neoadjuvant MAP chemo + limb-sparing wide excision + adjuvant chemo.
Pattern 2 — The Ewing question: Child/adolescent with diaphyseal lesion, onion-skin periosteum, large soft-tissue mass, fever, CD99-positive small round blue cells, t(11;22). Diagnosis? Ewing sarcoma. Treatment? VDC/IE chemo + local control (surgery and/or RT — Ewing is radiosensitive).
Pattern 3 — The chronic osteomyelitis question: Open fracture history, chronic discharging sinus, sequestrum + involucrum + cloaca on X-ray, S. aureus on culture. Diagnosis? Chronic osteomyelitis. Definitive treatment? Debridement, sequestrectomy, culture-guided antibiotics for 6 weeks, soft-tissue cover, bone reconstruction if defect.
Pattern 4 — The Paget question: Older adult with cotton-wool skull, picture-frame vertebra, bowed tibia, isolated raised serum ALP, deafness, headache. Diagnosis? Paget disease. Treatment? IV zoledronate 5 mg. Most feared complication? Secondary osteosarcoma (1 percent).
Pattern 5 — The GCT question: Skeletally mature adult with eccentric epiphyseal soap-bubble lytic lesion around the knee, multinucleated giant cells on biopsy. Diagnosis? Giant cell tumor. Treatment? Intralesional curettage with adjuvant; denosumab for unresectable; en bloc resection for Campanacci 3.
Pattern 6 — The matrix question: Identifies tissue of origin from radiographic matrix appearance. Cloud-like (osteoid) → bone-forming tumor (osteosarcoma). Rings and arcs / popcorn (chondroid) → cartilage tumor (enchondroma, chondrosarcoma, chondroblastoma). Ground-glass (fibrous) → fibrous dysplasia.
High-yield one-liners:
Use Lodwick or Enneking pattern analysis — six features. (1) Patient age — under 5 metastatic neuroblastoma/Ewing/eosinophilic granuloma; 5-30 osteosarcoma/Ewing/osteoblastoma; 30-40 GCT/chondrosarcoma; over 40 metastasis/multiple myeloma. (2) Location in the bone — epiphysis suggests GCT or chondroblastoma; metaphysis osteosarcoma/non-ossifying fibroma; diaphysis Ewing/lymphoma/fibrous dysplasia. (3) Margin — narrow zone of transition (well-defined sclerotic rim) is benign and slow-growing; wide zone of transition or moth-eaten/permeative pattern is aggressive. (4) Periosteal reaction — solid/buttress is benign; lamellated onion-skin, sunburst spiculated, or Codman triangle is aggressive. (5) Matrix mineralisation — chondroid (rings and arcs, popcorn) suggests cartilage tumor; osteoid (cloud-like) suggests bone-forming tumor; fibrous (ground-glass) suggests fibrous dysplasia. (6) Soft-tissue extension — present in aggressive tumors and infection.
Both are aggressive periosteal reactions but classically associate with different tumors. Codman triangle is a triangular elevation of periosteum at the edge of a lesion where the periosteum has been lifted by rapidly growing tumor and ossifies only at the edge — most classically described in osteosarcoma but also seen in Ewing sarcoma, infection, and subperiosteal hematoma. Onion-skin periosteal reaction is multilayered lamellated new bone formation parallel to the cortex, classically described in Ewing sarcoma but also in osteomyelitis and Langerhans cell histiocytosis. Sunburst (sunray) periosteal reaction is divergent spicules of new bone perpendicular to the cortex, very characteristic of osteosarcoma — caused by Sharpey fibres being elevated and ossified in radial orientation.
Chronic osteomyelitis classically shows a sequestrum (a fragment of dead, sclerotic, non-vascularised bone separated from healthy bone), an involucrum (new periosteal bone formation surrounding the sequestrum and forming a sleeve), and a cloaca (an opening in the involucrum through which pus and necrotic bone discharge to the soft tissues, often draining via a sinus tract to the skin). Additional findings: cortical thickening, mixed lytic-sclerotic appearance, soft-tissue swelling, and peri-osteal reaction. Brodie's abscess is a well-defined intramedullary lytic lesion with a sclerotic rim representing chronic localised osteomyelitis, often in the metaphysis of the tibia. CT defines sequestra and cloacae better than plain film; MRI defines marrow edema and abscess; nuclear medicine (bone scan, gallium, labelled WBC) is useful for activity assessment.
Paget disease has three radiographic phases. Lytic phase: well-defined V-shaped advancing lytic margin, classically described in long bones as 'blade of grass' or 'flame' appearance. Mixed (active) phase: coarsened trabeculae, cortical thickening, and bone enlargement. Sclerotic (burned-out) phase: dense bone with thickened trabeculae and cortex. Site-specific signs: cotton-wool appearance of the skull (multiple ill-defined sclerotic patches), picture-frame vertebra (thickened cortex around the vertebral body), ivory vertebra (uniformly dense vertebra — also seen in metastasis and lymphoma), tibial bowing (saber tibia), and skull base inversion / basilar invagination. Complications include pathological fracture, deafness (cranial nerve compression), high-output cardiac failure, and 1 percent risk of secondary osteosarcoma transformation. Raised serum alkaline phosphatase with normal calcium and phosphate is the biochemical signature.
Both are eccentric, expansile, lytic lesions but key features distinguish them. Giant cell tumor (GCT): age 20-40 (skeletally mature), epiphyseal location extending to subchondral bone (or metaphyseal-epiphyseal in skeletally immature), eccentric, expansile, well-defined non-sclerotic margin (narrow zone of transition without a sclerotic rim), classic 'soap-bubble' appearance from internal trabeculation, no matrix mineralisation, may have cortical breakthrough but no periosteal reaction typically. Most common sites: distal femur, proximal tibia (around the knee), distal radius. Aneurysmal bone cyst (ABC): age 5-20 (skeletally immature), metaphyseal location, eccentric, markedly expansile ('blown-out'), thin sclerotic rim with internal septations and characteristic fluid-fluid levels on MRI from blood components. ABC may be primary or secondary to another lesion (GCT, chondroblastoma, fibrous dysplasia). On MRI, both show fluid-fluid levels, but GCT also shows a solid component — differentiating from purely cystic ABC.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026