Version 1.0 — Published May 2026
Quick Answer
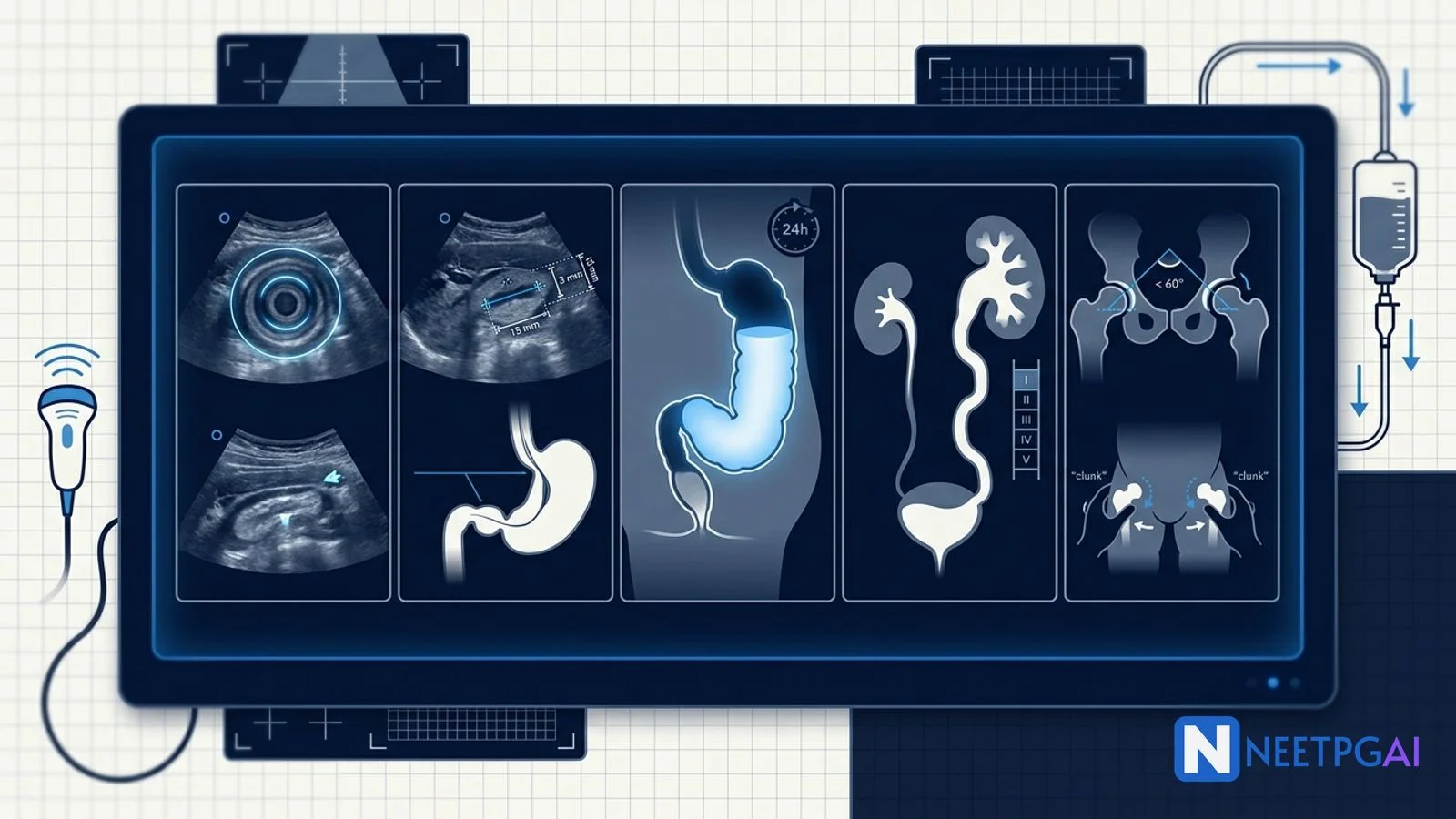
Pediatric imaging contributes 5-7 image-based MCQs per NEET PG paper, primarily under radiology, pediatrics, and surgery. Five high-yield patterns recur reliably year after year:
- Intussusception — target sign on transverse USG (concentric rings), pseudokidney sign on longitudinal; lesion greater than 2.5 cm; absent Doppler flow suggests ischaemia
- Hypertrophic pyloric stenosis (HPS) — pyloric muscle thickness greater than 3 mm, channel length greater than 15 mm on USG; string sign on UGI study (historic)
- Hirschsprung disease — transition zone on contrast enema; recto-sigmoid index less than 1; rectal biopsy is the gold-standard diagnostic
- Vesicoureteric reflux (VUR) — MCUG grading I-V (IRS classification); DMSA for renal scarring; prophylactic antibiotics for I-III, surgery for IV-V or breakthrough
- Developmental dysplasia of the hip (DDH) — Graf ultrasound alpha angle less than 60 degrees is abnormal; Ortolani-Barlow on examination; Pavlik harness under 6 months
Locking these 5 patterns plus 10-15 additional PYQ images (NEC pneumatosis intestinalis, congenital diaphragmatic hernia, biliary atresia, hydronephrosis) over 2-3 weeks moves accuracy from 40 to 80 percent in pediatric radiology MCQs.
Why pediatric imaging MCQs are high-yield for NEET PG
Pediatric imaging cuts across radiology, pediatrics, pediatric surgery, and urology. NEET PG, INI-CET, and FMGE feature pediatric imaging in 5-7 questions per paper, often coupled with a classical clinical vignette to test pattern recognition, age-appropriate diagnostic algorithms, and management decisions. Many of these conditions (intussusception, HPS, DDH) are common in Indian district hospitals where early diagnosis can prevent significant morbidity. The imaging patterns are stereotyped, reproducible, and frequently revisited in PYQs.
Drilling these 5 patterns plus 10-15 additional PYQ images over 2-3 weeks moves accuracy from 40 to 80 percent.
Foundational approach before the MCQs
Systematic pediatric imaging read
| Step | What to look at | Common abnormalities |
|---|
| Age and presentation | Age, sex, classic syndromic clue | Infants (HPS, intussusception, NEC), toddlers (intussusception, foreign body), older (appendicitis, VUR) |
| Modality | USG (first-line in infants — no radiation), X-ray, contrast study, MCUG, MRI, DMSA scan | Choose based on suspected pathology |
| Anatomy | Normal age-related anatomy (thymic shadow on CXR, ossification centres) | Atypical findings |
| Disease pattern | Target sign, transition zone, string sign, etc. | Pattern-based pediatric recognition |
| Severity grading | VUR grade I-V, Graf type I-IV, etc. | Management implications |
| Complications | Pneumatosis, perforation, ischaemia | Urgent intervention triggers |
Age-based mental shortlists for the pediatric abdomen
| Age | Common conditions | Imaging clue |
|---|
| Newborn (0-1 month) | Necrotising enterocolitis, malrotation/midgut volvulus, Hirschsprung, oesophageal atresia, congenital diaphragmatic hernia, biliary atresia | Pneumatosis intestinalis, whirlpool sign, transition zone, double bubble |
| Infant (1-12 months) | Hypertrophic pyloric stenosis, intussusception, GERD, UTI/VUR, DDH | Target sign, pyloric thickness, Graf alpha angle |
| Toddler (1-3 years) | Intussusception, foreign body, constipation, UTI/VUR | Target sign, foreign body silhouette, MCUG |
| School-age (3-12 years) | Appendicitis, Wilms tumour, neuroblastoma, septic arthritis | RIF mass, abdominal solid tumour, joint USG |
| Adolescent | Appendicitis, ovarian torsion, testicular torsion | Pattern recognition |
MCQ 1: 8-month-old infant with intermittent crying, vomiting, and red currant jelly stools
Image description: [Transverse abdominal ultrasound of an 8-month-old infant presenting with intermittent screaming episodes for 12 hours, vomiting (initially milk, then bilious), and passage of "red currant jelly" stools 2 hours before presentation. The ultrasound image shows a 4.2 cm diameter mass in the right upper quadrant just below the liver edge. On transverse section, the mass demonstrates the classic target sign (doughnut sign) — multiple alternating concentric hypoechoic and hyperechoic rings, representing the outer wall of the intussuscipiens, the dragged-in mesenteric fat (echogenic), and the inner wall of the intussusceptum. A longitudinal view of the same lesion shows the pseudokidney sign — a layered hypoechoic and hyperechoic structure resembling a kidney with central echogenic mesenteric fat. Colour Doppler shows preserved blood flow within the mass. A few mesenteric lymph nodes are seen within the intussusceptum. No free fluid.]
Clinical vignette: An 8-month-old previously healthy male infant is brought to the emergency department by his mother with a 12-hour history of episodic severe abdominal pain. The episodes last 3-5 minutes during which the baby screams, draws his knees up to his chest, and turns pale; between episodes he appears lethargic but otherwise well. He has vomited 6 times — initially milk feeds, then yellow-green bile-stained vomit in the last 2 hours. His mother noticed a "jelly-like dark red" substance in his diaper 2 hours ago. On examination: pulse 160/min, BP 88/52, RR 32/min, alert but lethargic. Abdomen — mildly distended, a sausage-shaped mass palpable in the right upper quadrant. Bowel sounds reduced. Per-rectal — empty rectum, blood-tinged mucus on the glove.
Options:
- (a) Intussusception
- (b) Midgut volvulus with malrotation
- (c) Meckel diverticulum with bleed
- (d) Necrotising enterocolitis
Correct answer: (a) Intussusception
Reasoning: The clinical triad of intermittent severe abdominal pain (colic), vomiting, and red currant jelly stools in an infant aged 3 months to 3 years is the classic presentation of intussusception. The palpable sausage-shaped mass in the right upper quadrant is Dance sign. Ultrasound shows the diagnostic target sign on transverse section and pseudokidney sign on longitudinal section, with the lesion measuring over 2.5 cm and preserved Doppler flow (no ischaemia yet — favourable for non-operative reduction). Most common location is ileocolic (90 percent). Most common age 5-10 months (peak 6-9 months). Most are idiopathic (lymphoid hyperplasia in Peyer patches following viral illness in over 90 percent of cases under 2 years).
Midgut volvulus would show the whirlpool sign of SMA-SMV mesenteric twisting on USG and double bubble or paucity of distal gas on X-ray, plus bilious vomiting from birth or early infancy — bilious vomit in an infant is malrotation until proven otherwise but our patient's symptom evolution and the target sign are diagnostic of intussusception. Meckel diverticulum bleeds painlessly — no colicky pain. NEC affects neonates (especially preterm) with pneumatosis intestinalis on X-ray.
Teaching pearl — non-operative reduction of intussusception:
- First-line treatment is pneumatic (air) or hydrostatic (saline) reduction under fluoroscopy or ultrasound guidance in haemodynamically stable patients with no peritonitis, no perforation, and no Doppler-detected ischaemia
- Air enema reduction success rate 80-90 percent with experienced operators
- Contraindications to non-operative reduction — peritonitis, perforation, ischaemia, haemodynamic instability, lead point identified (Meckel diverticulum, polyp, lymphoma, HSP gut wall haematoma)
- Recurrence after first reduction 5-10 percent, usually within 24 hours
- Surgical reduction (open or laparoscopic) reserved for failed non-operative reduction, contraindications above, or recurrent intussusception with lead point
MCQ 2: 4-week-old infant with non-bilious projectile vomiting and a palpable olive
Image description: [Transverse abdominal ultrasound of a 4-week-old male infant who has had progressive non-bilious projectile vomiting for 10 days, initially attributed to GERD but now occurring after every feed with a visible "olive" mass in the right upper quadrant. The ultrasound shows the pylorus with thickened hypoechoic muscle wall measuring 5.2 mm in single-wall thickness (over the diagnostic cut-off of 3 mm), and the pyloric channel length is 19 mm (over the 15 mm cut-off) on longitudinal view. The pyloric channel appears constantly closed with hyperperistalsis of the gastric antrum proximally. The stomach is markedly distended with retained fluid and food. A target appearance in transverse section shows the thickened muscle ring around the echogenic mucosa. A paired UGI barium study (historical) shows a thin "string sign" — a narrow string-like column of contrast passing through the elongated pyloric channel, with proximal antral bulging (shoulder sign) and a mushroom appearance of the duodenal cap.]
Clinical vignette: A 4-week-old male infant, first-born of non-consanguineous parents, is brought to the OPD with 10 days of vomiting after feeds. Initially the vomits were small and considered "spitting up", but over the past 4 days they have become forceful, projectile, and immediately post-feed. The vomitus is yellowish curdled milk — non-bilious. The baby is feeding eagerly between vomits ("hungry vomiter"). Weight has fallen from the birth weight 3.2 kg to the current 3.4 kg (well below the expected growth curve). On examination: appears slightly dehydrated, sunken fontanelle, dry mucous membranes. Pulse 158/min, BP 84/50. Abdomen — visible gastric peristalsis from left to right, a 1.5 cm firm "olive-like" mass palpable in the epigastrium just right of midline below the liver edge during a test feed. Bowel sounds present.
Lab — Na 132, K 3.0, Cl 86, HCO3 32, ABG pH 7.49, bicarb 32, pCO2 44 (hypochloraemic hypokalaemic metabolic alkalosis). Random blood glucose 64 mg/dL.
Options:
- (a) Hypertrophic pyloric stenosis (HPS)
- (b) Gastroesophageal reflux disease (GERD)
- (c) Pylorospasm
- (d) Antral web
Correct answer: (a) Hypertrophic pyloric stenosis (HPS)
Reasoning: Non-bilious projectile vomiting in a 3-8 week old infant with a hungry-vomiter appearance and a palpable "olive" mass is classic HPS. The diagnostic ultrasound criteria are met — pyloric muscle thickness 5.2 mm (over 3 mm) and channel length 19 mm (over 15 mm). The biochemistry shows the classic hypochloraemic hypokalaemic metabolic alkalosis from prolonged vomiting of HCl-rich gastric contents, with paradoxical aciduria as the kidney attempts to conserve sodium at the expense of hydrogen ions in late dehydration.
GERD would have vomits of smaller volume, not progressive, no olive mass, and normal biochemistry. Pylorospasm shows transient thickening that resolves on repeat scan and muscle thickness under 3 mm. Antral web is a rare congenital obstruction of the gastric antrum, presents earlier in the newborn period, and shows a fixed antral filling defect on UGI study — not the pyloric channel elongation.
Teaching pearl — Ramstedt pyloromyotomy:
- Definitive treatment is Ramstedt extramucosal longitudinal pyloromyotomy — a longitudinal seromuscular incision through the hypertrophied pylorus, leaving the mucosa intact
- Performed open (small RUQ transverse incision) or laparoscopically; outcomes equivalent
- Pre-operative correction of dehydration and metabolic alkalosis is MANDATORY before surgery (urine chloride over 20 mEq/L, serum bicarbonate under 30, serum chloride over 100) — alkalosis impairs respiratory drive on extubation
- Post-operative feeds resumed at 6-8 hours, full feeds by 24-48 hours
- Recovery rapid, mortality very low (under 0.5 percent), no long-term sequelae
MCQ 3: 4-month-old infant with failure to thrive and chronic constipation since birth
Image description: [Lateral contrast enema (water-soluble contrast, not barium) of a 4-month-old male infant. The image shows a markedly narrow distal rectum and rectosigmoid measuring approximately 1.5 cm in diameter with irregular contractions, transitioning at the level of the mid-sigmoid colon to a dilated proximal sigmoid colon measuring 4 cm in diameter. The transition zone is clearly visible as a funnel-shaped narrowing. The recto-sigmoid index (rectum diameter / sigmoid diameter) is 0.4 (less than 1) — inverted from the normal pattern. The dilated proximal sigmoid loops back upon itself with retained faecal material. Contrast retention is visible on a 24-hour delayed film showing significant proximal stasis.]
Clinical vignette: A 4-month-old male infant is brought to the pediatric outpatient department with chronic constipation since birth. He passed meconium on day 4 of life (normal infants pass meconium within 48 hours, mostly within 24). Bowel movements occur only every 5-7 days, often with significant straining and abdominal distension. His weight has plateaued at the 25th percentile (was 50th at birth). Recurrent abdominal distension with episodes of explosive watery foul-smelling stools — concerning for enterocolitis. On examination: abdomen distended, palpable faecal mass in the left lower quadrant. Per-rectal: empty rectum with explosive release of stool and gas on withdrawal of the examining finger (positive squirt sign). Anal tone normal.
Options:
- (a) Hirschsprung disease (congenital aganglionic megacolon)
- (b) Functional constipation
- (c) Anorectal malformation (low anomaly)
- (d) Hypothyroidism
Correct answer: (a) Hirschsprung disease (congenital aganglionic megacolon)
Reasoning: Delayed passage of meconium (after 48 hours), chronic constipation from birth, failure to thrive, abdominal distension, palpable faecal mass, an empty rectum on per-rectal, positive squirt sign, and the contrast enema showing a transition zone with recto-sigmoid index inverted (less than 1) plus 24-hour contrast retention is textbook short-segment Hirschsprung disease.
Functional constipation typically presents after weaning (4-12 months) or with toilet training (2-4 years), with stool retention in the rectum (full rectum on PR), and responds to dietary and laxative measures. Anorectal malformation would be diagnosed at birth examination. Hypothyroidism causes constipation but with characteristic features (large posterior fontanelle, prolonged jaundice, hypotonia, umbilical hernia) and is screened on the newborn dried blood spot.
Teaching pearl — definitive diagnosis and management:
- Definitive diagnosis is rectal biopsy showing absent ganglion cells in the submucosal (Meissner) and myenteric (Auerbach) plexuses, with hypertrophied nerve trunks and positive acetylcholinesterase staining (calretinin negative)
- Anorectal manometry shows absent rectoanal inhibitory reflex (RAIR) — useful in older children
- Treatment is staged — initial decompression by colostomy or rectal washouts; definitive pull-through surgery (Soave endorectal pull-through, Swenson pull-through, Duhamel retrorectal pull-through, or transanal endorectal pull-through TEPT) bringing ganglionated bowel down to the anus
- 75-80 percent are short-segment (rectum and rectosigmoid); 15-20 percent long-segment; under 5 percent total colonic
- Associations — Down syndrome (10 percent), MEN2A, Waardenburg syndrome, congenital deafness
MCQ 4: 3-year-old girl with recurrent febrile UTIs and renal scarring
Image description: [Micturating cystourethrogram (MCUG) of a 3-year-old female child with 4 documented urinary tract infections in the past 18 months. The image shows the bladder filled with contrast via a urethral catheter. During voiding, contrast is seen refluxing up the right ureter (tortuous and dilated), into a markedly dilated renal pelvis and calyces of the right kidney. The calyceal fornices are completely obliterated and the calyces appear blunted and dilated. The papillary impressions are mostly lost, with only a few preserved on the upper pole. The ureter is grossly tortuous with kinking. The left side appears normal with no reflux. A paired DMSA renal scan shows reduced uptake in the right upper pole (renal scarring) with split renal function 35 percent on the right and 65 percent on the left.]
Clinical vignette: A 3-year-old female child is referred to the pediatric nephrology clinic after her fourth febrile UTI in 18 months (all E coli on culture, two requiring hospitalisation for IV antibiotics). She is otherwise well, age-appropriate development, normal voiding pattern, no incontinence, no constipation. Family history — her elder sister had a similar history (VUR Grade IV that resolved spontaneously by age 7). Examination — afebrile today, abdomen soft, no palpable masses, normal external genitalia, normal lower back (no sacral dimple or tuft). Urine routine today: clear, no growth.
Options:
- (a) Vesicoureteric reflux Grade V — needs surgical correction
- (b) Vesicoureteric reflux Grade III — continue prophylactic antibiotics
- (c) Posterior urethral valves
- (d) Pelviureteric junction obstruction
Correct answer: (a) Vesicoureteric reflux Grade V — needs surgical correction
Reasoning: The MCUG demonstrates gross dilatation and tortuosity of the ureter, gross dilatation of the renal pelvis and calyces, complete obliteration of the fornices, and loss of papillary impressions in the majority of calyces — these are the defining features of VUR Grade V (International Reflux Study classification). DMSA scan confirms renal scarring with reduced split function. Grade V VUR has a low spontaneous resolution rate (under 30 percent) and high risk of progressive renal scarring; surgical intervention (ureteric reimplantation by Cohen cross-trigonal, Politano-Leadbetter, or Lich-Gregoir extravesical technique, or endoscopic Deflux injection in milder cases) is recommended.
Grade III VUR shows mild to moderate dilatation only (not gross). Posterior urethral valves are a male-only diagnosis (membranous obstruction in the posterior urethra) and would show a dilated posterior urethra on MCUG with bladder trabeculation. PUJ obstruction shows hydronephrosis without ureteric dilatation on USG.
Teaching pearl — VUR grading IRS:
| Grade | MCUG appearance | Management |
|---|
| I | Reflux into ureter only, no dilatation | Antibiotic prophylaxis, observe |
| II | Reflux up to renal pelvis, no dilatation | Antibiotic prophylaxis, observe |
| III | Mild-moderate dilatation of ureter, pelvis, calyces; minimal forniceal blunting | Antibiotic prophylaxis; surgery if breakthrough |
| IV | Moderate ureteric tortuosity; moderate pelvic-calyceal dilatation; obliterated fornices; preserved papillae | Often surgery, especially with scarring |
| V | Gross ureteric tortuosity; gross pelvic-calyceal dilatation; lost papillae | Surgery — reimplantation |
- Initial workup of UTI in children — ultrasound for all febrile UTIs; MCUG for atypical UTI, recurrence, or USG abnormality; DMSA at 4-6 months post-infection for cortical scarring assessment
- Antibiotic prophylaxis — cotrimoxazole, nitrofurantoin, or cefixime once daily (one-quarter therapeutic dose); duration variable but typically until age 5 or VUR resolution
- Surveillance — annual blood pressure (HTN from renal scarring), urine routine, ultrasound; renal function (creatinine, eGFR) periodically
MCQ 5: 6-week-old breech-delivered female infant with asymmetric skin creases and limited hip abduction
Image description: [Coronal hip ultrasound (Graf technique) of a 6-week-old female infant. The image shows the left hip in coronal section through the deepest part of the acetabulum. The bony acetabular roof appears shallow. The alpha angle measures 48 degrees (normal greater than or equal to 60 degrees; type IIc in Graf classification at this age would be 43-49 degrees, type D 43-49 with eccentric femoral head). The femoral head appears subluxated laterally with the bony cartilage interface displaced. The labrum (cartilaginous roof) is everted superolaterally. The beta angle (cartilaginous roof angle) measures 78 degrees (normal less than 55-77 depending on type). A paired AP X-ray of the pelvis (taken later at 8 months) shows the right femoral head ossification centre but the left absent, with a broken Shenton line (the arc from the medial femoral neck to the superior obturator foramen is discontinuous), the left femoral epiphysis is in the upper outer quadrant of the Hilgenreiner-Perkin grid, and the acetabular index on the left is 36 degrees (over 30 degrees abnormal).]
Clinical vignette: A 6-week-old first-born female infant is brought for routine well-baby visit. She was delivered by elective LSCS at 38 weeks for breech presentation and oligohydramnios. Birth weight 2.8 kg. No family history. The mother has noticed asymmetric skin creases on the medial thigh — three creases on the left vs two on the right — and that the left leg "looks shorter than the right" when the baby lies on her back. On examination: weight on track, age-appropriate. Hip examination — limited abduction on the left (60 degrees vs 80 degrees on the right). Galeazzi sign positive — when the infant lies supine with hips and knees flexed, the left knee is lower than the right. Ortolani test positive — a palpable "clunk" of reduction when the left hip is abducted (the dislocated femoral head reduces over the posterior acetabular rim). Barlow test positive on the left.
Options:
- (a) Developmental dysplasia of the hip (DDH) — needs Pavlik harness
- (b) Septic arthritis of the hip
- (c) Transient synovitis of the hip
- (d) Slipped capital femoral epiphysis
Correct answer: (a) Developmental dysplasia of the hip (DDH) — needs Pavlik harness
Reasoning: All five classic DDH risk factors and signs are present — female (4:1 female-to-male predominance), first-born, breech presentation, oligohydramnios, asymmetric skin creases, positive Galeazzi sign, positive Ortolani test (palpable clunk of reduction), positive Barlow test (provocable dislocation), and limited abduction. Graf ultrasound confirms — alpha angle 48 degrees (less than 60), everted labrum, lateral subluxation — Graf type III dysplasia (dislocated with everted labrum). The infant is well-developed otherwise.
Septic arthritis would present with fever, refusal to move the limb, pseudoparalysis, raised WBC/CRP, and joint effusion on USG with restricted movement throughout. Transient synovitis affects 3-8 year olds (not 6-week-olds), follows a viral illness, and resolves in 1-2 weeks. Slipped capital femoral epiphysis is a disease of adolescents (10-16 years), often obese.
Teaching pearl — DDH management by age:
- 0-6 months — Pavlik harness (dynamic abduction splint) for type IIc and above, worn 23 hours per day; check ultrasound at 3-6 weeks; success rate 85-95 percent if started under 3 months
- 6-18 months — closed reduction under general anaesthesia and spica cast immobilisation in the "human position" (90 degrees flexion, 40-60 degrees abduction); arthrogram to confirm concentric reduction; cast for 3-6 months
- Over 18 months — open reduction with capsulorrhaphy +/- femoral or pelvic osteotomy (Salter, Pemberton, Dega, or Chiari) to remodel the dysplastic acetabulum
- Pavlik harness contraindications — type IV irreducible dislocation, neuromuscular disease (cerebral palsy), age over 6 months
- Complications — avascular necrosis of femoral head (3-30 percent depending on technique), residual subluxation needing later osteotomy, recurrence
Common pitfalls in pediatric imaging MCQs
Five frequent error patterns appear in NEET PG dissection of pediatric image MCQs.
Pitfall 1: Mixing up target sign and pseudokidney sign
The target sign (doughnut sign) is seen on transverse section of an intussusception — concentric rings. The pseudokidney sign is seen on longitudinal section of the same lesion — layered structure resembling a kidney. Both refer to intussusception in different planes. Some examiners use them interchangeably and others test the distinction.
Pitfall 2: Confusing 3 mm vs 4 mm for pyloric muscle thickness
The diagnostic cut-off for hypertrophic pyloric stenosis is pyloric muscle thickness greater than or equal to 3 mm (some institutions use 4 mm as the higher specificity cut-off, others 3 mm as the higher sensitivity cut-off). NEET PG most commonly tests 3 mm. Channel length cut-off is 15 mm. Borderline cases (2.5-3 mm thickness) need repeat scan in 24-48 hours.
Pitfall 3: Forgetting that contrast enema is not the gold standard for Hirschsprung
Contrast enema shows the transition zone but is NOT diagnostic — rectal biopsy is the gold-standard. NEET PG sometimes asks "investigation of choice" — answer is rectal biopsy (suction biopsy or full-thickness), not contrast enema. Anorectal manometry showing absent RAIR is a useful adjunct in older children.
Pitfall 4: Confusing VUR grading on MCUG
The IRS grading is I to V. Grade I — ureter only, no dilatation. Grade II — pelvis and ureter, no dilatation. Grade III — mild-moderate dilatation, minimal forniceal blunting. Grade IV — obliterated fornices, preserved papillae. Grade V — gross dilatation, lost papillae. Common error is upgrading Grade III to Grade IV — remember Grade IV needs fornices obliterated.
Pitfall 5: Confusing alpha and beta angles in Graf classification
Alpha angle measures bony acetabular coverage — formed between the bony acetabular line and the iliac wing line. Normal alpha greater than or equal to 60 degrees. Lower alpha = more dysplastic. Beta angle measures cartilaginous coverage — between the cartilaginous roof and iliac wing line. Normal beta less than 55 degrees (some sources less than 77 depending on Graf type). Higher beta = more dysplastic. NEET PG most commonly tests alpha 60 degrees as the diagnostic cut-off.
How to study pediatric imaging for NEET PG
- Memorise the 5 patterns in this article cold — target sign, pyloric criteria, Hirschsprung transition zone, VUR grading I-V, Graf alpha angle
- Review 10-15 additional PYQ images — NEC pneumatosis intestinalis, midgut volvulus whirlpool sign, congenital diaphragmatic hernia bowel in chest, biliary atresia triangular cord sign, hydronephrosis grading, posterior urethral valves dilated posterior urethra, neural tube defects, congenital heart disease (boot-shaped heart, egg-on-side, snowman)
- Pair images with classic vignettes — age, sex, symptom triad, signs, labs — so pattern recognition triggers automatically
- Use spaced repetition — 1d, 3d, 7d, 14d, 30d review of the same 25-30 high-yield pediatric images
- Practice in the question bank — NEETPGAI offers a tagged pediatric imaging set; do 20-30 questions per day for 2-3 weeks
Key takeaways
- Pediatric imaging contributes 5-7 image MCQs per NEET PG paper
- USG is first-line in infants (no radiation); X-ray, contrast study, MCUG, DMSA scan, MRI based on suspected pathology
- Intussusception — target sign (transverse), pseudokidney sign (longitudinal); air enema reduction if stable
- HPS — pyloric muscle over 3 mm, channel over 15 mm; correct alkalosis before Ramstedt pyloromyotomy
- Hirschsprung — transition zone on contrast enema, recto-sigmoid index less than 1; rectal biopsy is gold standard
- VUR — IRS grading I-V on MCUG; prophylactic antibiotics for I-III, surgery for IV-V
- DDH — Graf ultrasound alpha less than 60 degrees abnormal; Pavlik harness under 6 months
- Pair images with classic vignettes for fast pattern recognition
Frequently Asked Questions
What are the ultrasound criteria for intussusception and how are they distinguished from other causes of abdominal pain in infants?
Ultrasound is the gold-standard investigation for intussusception in children, with sensitivity 97-100 percent and specificity 88-100 percent. The classic findings are the target sign (or doughnut sign) on transverse section — alternating concentric hypoechoic and hyperechoic rings representing the outer intussuscipiens and inner intussusceptum with mesenteric fat dragged in — and the pseudokidney sign on longitudinal section, where the layered structure resembles a kidney with central echogenic mesenteric fat. The lesion is typically over 2.5 cm in diameter (smaller transient small-bowel intussusceptions are often physiological and self-resolving). Additional findings are free fluid, lymph nodes within the intussusceptum, and absent blood flow on colour Doppler (suggesting ischaemia, which is a contraindication to non-operative reduction). Differentials in an infant with intermittent abdominal pain, vomiting, and red currant jelly stools include gastroenteritis (diffuse bowel oedema, no target sign), midgut volvulus (whirlpool sign of SMA-SMV around the mesentery), Meckel diverticulum bleed (Tc-99m pertechnetate scan), and HSP (rash, joint pain). NEET PG tests the target and pseudokidney signs in nearly every pediatric imaging set.
What is the ultrasound definition of hypertrophic pyloric stenosis (HPS) and what does the string sign on UGI study mean?
Hypertrophic pyloric stenosis presents classically at 3-6 weeks of age (range 2-8 weeks) with non-bilious projectile vomiting, palpable olive in the right upper quadrant, and visible gastric peristalsis. The diagnostic imaging is abdominal ultrasound. The diagnostic criteria are pyloric muscle thickness greater than 3 mm (single wall measurement in transverse view, classic 4-6 mm), pyloric channel length greater than 15 mm, and a target appearance in transverse section with thickened hypoechoic muscle around an echogenic mucosa. Failure of relaxation, hyperperistalsis, and gastric distension are dynamic findings. The string sign refers to the appearance on an upper gastrointestinal (UGI) barium study or contrast study, where a thin string-like channel of contrast is seen passing through the elongated pyloric channel — historically diagnostic but now largely replaced by ultrasound. Other signs on UGI include the shoulder sign (bulging of hypertrophied pyloric muscle into the antrum), the beak sign, and the mushroom sign. Differentials include pylorospasm (transient, normal muscle thickness under 3 mm), gastroesophageal reflux, milk protein intolerance, and metabolic disorders. NEET PG tests the 3 mm and 15 mm cut-offs, the projectile non-bilious vomiting, and the classic hypochloraemic hypokalaemic metabolic alkalosis pattern.
How is Hirschsprung disease diagnosed by contrast enema and what is the role of rectal biopsy?
Hirschsprung disease (congenital aganglionic megacolon) is caused by failed migration of neural crest cells along the gut tube, resulting in absence of ganglion cells in the submucosal Meissner and myenteric Auerbach plexuses of the affected distal bowel. The aganglionic segment is contracted, with the proximal bowel becoming dilated from chronic obstruction. Contrast enema (water-soluble contrast preferred over barium to minimise inspissation in already obstructed bowel) shows a classic transition zone — a narrow distal aganglionic segment (rectum and rectosigmoid in 75-80 percent of cases — short-segment disease) with proximal dilated bowel. The recto-sigmoid index (RSI = maximal rectal diameter divided by maximal sigmoid diameter) less than 1 is highly suggestive (in normal infants the rectum is larger than the sigmoid; in Hirschsprung, the dilated proximal sigmoid is larger). Other signs are irregular spasms in the aganglionic segment, retained contrast at 24 hours, and a serrated mucosal pattern in the transition zone. However, contrast enema alone is not diagnostic — definitive diagnosis is by rectal suction biopsy or full-thickness rectal biopsy showing absent ganglion cells and hypertrophied nerve trunks in the submucosa with positive acetylcholinesterase staining. Anorectal manometry shows absent rectoanal inhibitory reflex (RAIR). NEET PG tests the transition zone, the RSI inversion, and the gold-standard rectal biopsy.
What is the grading of vesicoureteric reflux on MCUG and what are the management implications?
Vesicoureteric reflux (VUR) is graded I to V on the International Reflux Study (IRS) classification, demonstrated by micturating cystourethrogram (MCUG, also called voiding cystourethrography VCUG). Grade I — reflux limited to the ureter, no dilatation. Grade II — reflux up to the renal pelvis without dilatation. Grade III — mild to moderate dilatation of the ureter, renal pelvis, and calyces; no or slight blunting of the fornices. Grade IV — moderate dilatation and tortuosity of the ureter; moderate dilatation of the renal pelvis and calyces with complete obliteration of fornices but preservation of papillary impressions in the majority. Grade V — gross dilatation and tortuosity of the ureter; gross dilatation of the renal pelvis and calyces; loss of papillary impressions in the majority of calyces. Management is graded — Grades I-II resolve spontaneously in 70-80 percent of cases by age 5, manage with continuous prophylactic antibiotics (cotrimoxazole or nitrofurantoin) and observation. Grade III variable, depends on age and breakthrough UTIs. Grades IV-V have lower spontaneous resolution (less than 30 percent), often need surgery — ureteric reimplantation (Cohen, Politano-Leadbetter, or Lich-Gregoir) or endoscopic Deflux injection. NEET PG tests grading, the role of DMSA for renal scarring assessment, and the indication for surgery.
How is developmental dysplasia of the hip (DDH) assessed on ultrasound and X-ray and what is the role of the alpha angle?
Developmental dysplasia of the hip (DDH) is assessed by ultrasound in infants under 6 months (femoral head not yet ossified) and by X-ray after 6 months. Graf ultrasound classification is the gold standard for infants under 6 months. The alpha angle measures bony acetabular roof depth — formed between the bony acetabular line and the iliac wing line (vertical cortex of the ilium). Normal alpha angle is greater than or equal to 60 degrees. Graf type I — normal hip (alpha greater than 60 degrees, mature). Graf type IIa — physiologically immature in under 3 months (alpha 50-59). Graf type IIb — pathological in over 3 months (alpha 50-59). Graf type IIc — critically dysplastic (alpha 43-49). Graf type D — decentred (alpha 43-49, beta over 77, eccentric femoral head). Graf type III — dislocated with everted labrum. Graf type IV — dislocated with inverted labrum. Other useful indices are the Reimer migration percentage (extent of femoral head lateral to Perkin vertical line), the acetabular index on X-ray (after 6 months, less than 30 degrees normal in newborns reducing to 22 degrees by 2 years), and the Shenton line on X-ray (continuous arc from medial femoral neck to superior obturator foramen, broken in DDH). Examination findings — Ortolani (reduction of dislocated hip on abduction), Barlow (provocation of dislocation on adduction with posterior pressure), Galeazzi (asymmetric knee heights), and limited abduction. Management — Pavlik harness under 6 months, closed reduction with spica cast 6-18 months, open reduction beyond 18 months. NEET PG tests the 60-degree alpha cut-off and the Graf classification heavily.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026