Quick Answer
Neonatal jaundice delivers 2 to 3 NEET PG questions per year across pediatrics and community medicine. Lock these:
- Physiological — after 24 h, unconjugated, peak day 3-5, TSB under 15 mg/dL term, resolves by day 14.
- Pathological — first 24 h, TSB over 95th percentile (Bhutani), rise over 5 mg/dL/day, direct over 2 mg/dL, prolonged.
- Bhutani nomogram — hour-specific TSB percentile drives phototherapy decision.
- Phototherapy — blue LED at 460 nm converts bilirubin to lumirubin (water-soluble).
- Exchange transfusion — TSB above threshold, B/A ratio over 8, kernicterus signs — double volume.
- Kernicterus — basal ganglia staining; choreoathetoid CP + upgaze palsy + deafness.
- India — G6PD deficiency common, birth-dose HBV, universal Rh-D immunoprophylaxis.
Neonatal hyperbilirubinemia is the pediatrics examiner's favourite hour-specific decision-tree question — it forces you to plot a TSB against a nomogram, calculate a bilirubin-to-albumin ratio, distinguish unconjugated from conjugated on a split-bilirubin, and choose between phototherapy and exchange transfusion. The trap-heavy zones are the biliary-atresia timing window, the phototherapy versus exchange-transfusion threshold, and the G6PD screening layer that Indian question banks now emphasise.
This NEETPGAI deep dive walks through the physiology of neonatal bilirubin metabolism, the physiological-versus-pathological distinction, unconjugated versus conjugated causes, the Bhutani nomogram and AAP 2022 hour-specific curves, phototherapy and exchange-transfusion algorithms, and kernicterus — with India-specific context on G6PD, Rh-D immunoprophylaxis and biliary-atresia timing.
Bilirubin metabolism — neonatal quirks
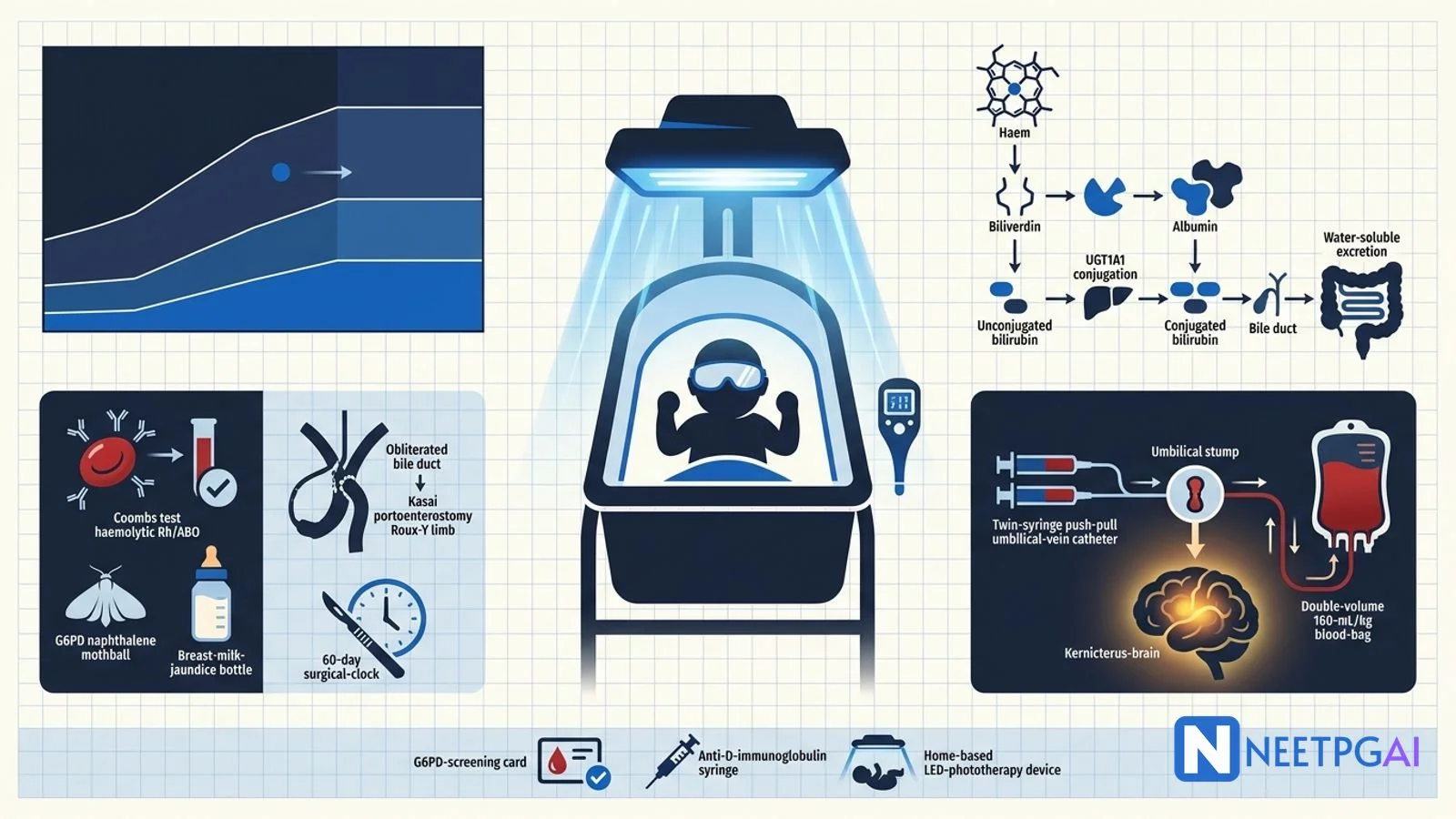
RBC breakdown releases haem → biliverdin → unconjugated bilirubin (bound to albumin in plasma). Hepatic uptake is followed by conjugation with glucuronic acid by UDP-glucuronosyltransferase (UGT1A1) to water-soluble conjugated bilirubin, excreted in bile. In the neonate, three factors raise unconjugated bilirubin:
- UGT1A1 immaturity — full activity by 6 to 14 weeks.
- Shorter RBC lifespan — about 90 days versus adult 120.
- Increased enterohepatic circulation — no gut flora yet, higher beta-glucuronidase in meconium, deconjugates bile back to unconjugated bilirubin, reabsorbed.
Physiological jaundice
- Appears after 24 hours.
- Unconjugated.
- Peaks on day 3 to 5 at under 15 mg/dL (term) or 17 mg/dL (preterm).
- Rise less than 5 mg/dL per day.
- Resolves by day 14 term / 21 preterm.
Breastfeeding-associated jaundice subtypes:
- Breastfeeding failure jaundice (early, first week) — inadequate intake, dehydration, weight loss, increased enterohepatic recirculation. Fix by feeding support, not stopping breast milk.
- Breast-milk jaundice (late, 5-14 days, may persist 3-12 weeks) — beta-glucuronidase in breast milk deconjugates bile bilirubin. Continue breastfeeding; only stop briefly for diagnostic uncertainty.
Pathological jaundice — flagging criteria
Any of the following makes jaundice pathological:
- Onset in the first 24 hours of life.
- TSB above the 95th percentile on the Bhutani nomogram at that age.
- Rise over 5 mg/dL per day.
- Direct bilirubin over 2 mg/dL or over 20 percent of TSB.
- Jaundice persisting past 14 days term / 21 days preterm.
- Clinical instability, sepsis or signs of BIND.
Unconjugated hyperbilirubinemia — causes
Haemolytic
- Rh isoimmunisation — Rh-negative mother, Rh-positive fetus, direct Coombs positive. Prevention — anti-D immunoglobulin at 28 weeks and within 72 hours postnatal.
- ABO incompatibility — group O mother, group A or B baby; direct Coombs weakly positive or negative; less severe than Rh.
- G6PD deficiency — X-linked, common in India (5-15 percent prevalence); triggered by naphthalene, sulpha drugs, fava beans; screened by NNS in high-prevalence regions.
- Hereditary spherocytosis — MCHC elevated, osmotic fragility positive, spherocytes on smear.
- Sepsis — hyperbilirubinaemia may be first sign.
Non-haemolytic
- Physiological.
- Breastfeeding failure and breast-milk jaundice.
- Crigler-Najjar syndrome — UGT1A1 mutations. Type I (complete deficiency, autosomal recessive, TSB over 20 mg/dL from day 1, unresponsive to phenobarbital, needs phototherapy and eventual liver transplant); Type II (partial deficiency, autosomal dominant with variable penetrance, milder, phenobarbital-responsive).
- Gilbert syndrome — UGT1A1 promoter polymorphism, mild intermittent unconjugated jaundice, benign — clinically silent in neonates.
- Extravascular blood — cephalhaematoma, subgaleal haemorrhage, bruising — heavy haem load, delayed peak.
- Polycythaemia — venous haematocrit over 65 percent.
- Congenital hypothyroidism — often prolonged unconjugated jaundice.
Conjugated hyperbilirubinemia — always pathological
Direct fraction over 2 mg/dL (or over 20 percent of TSB) is never physiological. Split bilirubin every jaundiced neonate beyond 14 days.
- Biliary atresia — most urgent; obliterative destruction of extrahepatic bile ducts; Kasai portoenterostomy before 60 days for best outcome.
- Choledochal cyst — Todani classification; type I most common.
- Neonatal hepatitis — idiopathic, TORCH, HIV.
- Alpha-1 antitrypsin deficiency — PiZZ genotype.
- Galactosaemia — GALT deficiency; jaundice + cataracts + hepatomegaly + E. coli sepsis; galactose-free formula.
- Tyrosinaemia — succinylacetone in urine; nitisinone treatment.
- Progressive familial intrahepatic cholestasis (PFIC) — types 1, 2, 3.
- TPN cholestasis — in preterms on prolonged parenteral nutrition.
Assessment
- Kramer rule — clinical assessment; jaundice progresses cephalocaudally in five zones — face (about 5 mg/dL), upper trunk (10), lower trunk-thighs (12), arms-lower legs (15), palms-soles (over 15). Poorly reliable — use TSB or transcutaneous bilirubin.
- Transcutaneous bilirubin (TcB) — screening; if in the high-intermediate or high-risk zone, confirm with serum TSB.
- Serum TSB — plot on Bhutani nomogram against hours of age.
- Investigations — CBC, reticulocyte count, blood group and Rh (mother and baby), direct Coombs, peripheral smear, split bilirubin, LFT, G6PD screen, TSH (if prolonged), urine culture, TORCH serology (if suggestive).
Bhutani nomogram + AAP 2022 curves
- Bhutani nomogram — hour-specific TSB percentile plot (24-168 hours).
- AAP 2022 — replaces 2004 curves; provides phototherapy and exchange-transfusion thresholds by hour, gestational age (35-37 weeks vs over 38) and risk factors (isoimmune haemolysis, G6PD, asphyxia, sepsis, albumin under 3 g/dL).
Escalation zones on Bhutani
- Under 40th percentile — low risk.
- 40-75th — low-intermediate.
- 75-95th — high-intermediate (repeat TSB in 6-12 h).
- Over 95th — high risk (start phototherapy).
Phototherapy
Mechanism — blue light at 460 nm (bilirubin absorption peak) converts fat-soluble unconjugated bilirubin to water-soluble isomers, excreted without conjugation:
- Configurational isomerisation (4Z,15Z → 4Z,15E) — rapid, reversible.
- Structural isomerisation to lumirubin — irreversible, main excretion route.
- Photo-oxidation — slow, minor.
Devices — LED (over 30 microwatts/cm2/nm, best); CFL (5-20); fibre-optic blankets for outpatient. Intensive phototherapy uses two or more devices simultaneously.
Standard care during phototherapy
- Eye shields.
- Increase fluids by 15-25 percent (insensible loss up).
- Continue breastfeeding.
- Repeat TSB in 4-6 h then 8-12 h.
- Stop when TSB is 2-3 mg/dL below the phototherapy line.
Complications — hyperthermia, dehydration, loose stools, transient rash, retinal damage without eye shields, separation from mother, DNA damage (rare, low-birth-weight preterm). Contraindicated in conjugated hyperbilirubinemia — bronze-baby syndrome (dark grey-brown discolouration, benign but ugly).
Exchange transfusion
Indications:
- TSB above the exchange-transfusion line on AAP 2022.
- B/A ratio over 8 (or over 7.2 in preterm).
- Rise over 1 mg/dL/hour despite intensive phototherapy.
- Any acute BIND signs (hypertonia, opisthotonus, high-pitched cry).
- Hydrops fetalis at birth from Rh isoimmunisation.
Technique
- Double-volume exchange — 160 mL/kg (twice the neonatal blood volume of 80 mL/kg).
- Cross-matched, irradiated, CMV-negative packed cells with fresh AB plasma.
- Umbilical vein catheter; isovolumetric (push-pull) via twin syringes.
- Removes about 85 percent of circulating unconjugated bilirubin and 25 percent of tissue-bound bilirubin.
Complications — thromboembolism, air embolism, portal vein thrombosis, sepsis, NEC (in preterms), thrombocytopenia, hyperkalaemia, hypocalcaemia, hypoglycaemia, arrhythmias, hypothermia.
Kernicterus (BIND)
Unconjugated bilirubin crosses the BBB and stains the basal ganglia (especially globus pallidus), hippocampus and subthalamic nuclei.
Acute BIND
- Phase 1 (first 1-2 days) — lethargy, poor feeding, hypotonia.
- Phase 2 (mid) — hypertonia, opisthotonus, retrocollis, high-pitched cry, fever.
- Phase 3 (advanced) — apnoea, seizures, death.
Chronic BIND
- Choreoathetoid cerebral palsy.
- Upgaze palsy (setting-sun sign).
- Sensorineural hearing loss (auditory neuropathy pattern — abnormal ABR with normal OAE).
- Enamel dysplasia (green teeth).
NEET PG MCQ traps
- Physiological jaundice — after 24 h, unconjugated, peak day 3-5, TSB under 15 mg/dL.
- Pathological — first 24 h, or rise over 5 mg/dL/day, or direct over 2 mg/dL, or prolonged.
- Rh isoimmunisation — direct Coombs positive.
- ABO incompatibility — direct Coombs weak positive or negative.
- G6PD deficiency — X-linked; common in India; naphthalene trigger.
- Crigler-Najjar Type I — complete UGT1A1 deficiency; not phenobarbital-responsive; liver transplant.
- Crigler-Najjar Type II — partial UGT1A1 deficiency; phenobarbital-responsive.
- Gilbert syndrome — mild UGT1A1 promoter defect; benign.
- Breastfeeding jaundice = early (first week, from inadequate intake).
- Breast-milk jaundice = late (over 7 days, beta-glucuronidase in milk).
- Bhutani nomogram — hour-specific percentile plot from 24-168 hours.
- AAP 2022 — updated hour-specific phototherapy and exchange-transfusion curves.
- Phototherapy peak wavelength = 460 nm (blue light).
- Lumirubin = major water-soluble excretion product of phototherapy.
- Bronze-baby syndrome — do not phototherapy conjugated hyperbilirubinemia.
- Kramer rule — cephalocaudal jaundice progression by zones; not reliable enough for treatment decisions.
- Exchange transfusion — double-volume 160 mL/kg; B/A ratio over 8; acute BIND signs.
- Biliary atresia — Kasai portoenterostomy before 60 days for best outcome.
- Split bilirubin every jaundiced neonate beyond 14 days.
- Choledochal cyst — Todani classification; type I most common.
- Galactosaemia — GALT deficiency; jaundice + cataracts + hepatomegaly + E. coli sepsis.
- Kernicterus stains basal ganglia (globus pallidus), hippocampus, subthalamic nuclei.
- Chronic BIND — choreoathetoid CP + upgaze palsy + sensorineural deafness + green teeth.
- Anti-D immunoglobulin — 28 weeks and within 72 h of delivery.
- India — G6PD common; universal Rh-D immunoprophylaxis; birth-dose HBV.
Recent updates and India context
- AAP 2022 hyperbilirubinemia guidelines — updated hour-specific phototherapy and exchange-transfusion thresholds; higher thresholds than 2004 (fewer phototherapy starts) with structured pre-discharge risk assessment.
- IAP (Indian Academy of Pediatrics) National Neonatology Forum (NNF) — endorses AAP 2022 curves for term and near-term, with adjustments for G6PD and preterm.
- National Neonatal Screening (NNS) — G6PD deficiency screening rolling out in high-prevalence states (Gujarat, Rajasthan, Andhra Pradesh, Karnataka, Tamil Nadu); congenital hypothyroidism, CAH, sickle cell and haemoglobinopathies covered nationally.
- Universal Rh-D immunoprophylaxis — anti-D at 28 weeks and within 72 hours postnatal is national ANC standard; free under NHM.
- Birth-dose hepatitis B vaccine — in UIP since 2011; national coverage over 80 percent.
- Home-based phototherapy — low-cost LED devices (Firefly, Brilliance) rolled out at PHC and Anganwadi level in high-burden districts.
- Kasai portoenterostomy centres — SGPGI Lucknow, ILBS Delhi, PGIMER Chandigarh, CMC Vellore, Apollo Delhi/Chennai, Kokilaben Mumbai, Narayana Bangalore. Liver-transplant back-up available at ILBS, Apollo, Medanta.
- National guideline — every neonate must be checked for jaundice at discharge, again on day 3, day 5-7 and day 14 by ASHA / ANM / paediatrician.
- India-specific G6PD trigger education — hospital-discharge counselling avoids naphthalene mothballs, sulpha, primaquine, fava beans in known cases.
- NNF 2020 protocol — Bhutani plus AAP-adapted thresholds; phototherapy starts at high-intermediate zone if any risk factor (isoimmune haemolysis, G6PD, asphyxia, sepsis, prematurity, hypoalbuminemia).
Frequently asked questions
What separates physiological from pathological neonatal jaundice?
Physiological jaundice is unconjugated, appears after 24 hours of life, peaks on day 3 to 5 at under 15 mg/dL in term babies (17 mg/dL in preterm), rises less than 5 mg/dL per day and resolves by day 14 in term or day 21 in preterm. Its mechanism is a triad — immature glucuronosyltransferase (UGT1A1), a shorter RBC lifespan (about 90 days versus adult 120) and increased enterohepatic recirculation. Pathological jaundice fails any of these criteria — jaundice in the first 24 hours, TSB above the 95th percentile on the Bhutani nomogram, rise over 5 mg/dL per day, direct fraction over 2 mg/dL (or over 20 percent of TSB) or jaundice persisting past those durations. Any pathological jaundice mandates a full workup starting with maternal blood group, Coombs test, CBC, reticulocyte count and peripheral smear.
How does the Bhutani nomogram guide phototherapy?
The Bhutani nomogram (1999) plots hour-specific total serum bilirubin (TSB) against age in hours from 24 to 168 hours, dividing infants into low, low-intermediate, high-intermediate and high-risk zones based on the 40th, 75th and 95th percentiles. The AAP 2022 hour-specific threshold curves (an update of the 2004 curves) then plot phototherapy and exchange-transfusion thresholds against age, gestational age (35 to 37 weeks versus 38 or more) and risk factors (isoimmune haemolysis, G6PD deficiency, asphyxia, sepsis). A term healthy baby at 48 hours with TSB 15 mg/dL is in the high-intermediate zone and needs phototherapy; the same baby at 96 hours with the same TSB is closer to the phototherapy line but on the border and warrants a repeat in 6 to 12 hours.
How does blue-light phototherapy convert bilirubin?
Blue-light phototherapy at 460 to 490 nm (peak absorption of bilirubin at 460 nm) converts fat-soluble unconjugated bilirubin in the skin into water-soluble isomers by three mechanisms — configurational isomerisation (rapid, reversible; converts 4Z,15Z bilirubin to 4Z,15E, excreted in bile without conjugation), structural isomerisation (irreversible; converts to lumirubin, the main excretion route in urine and bile) and photo-oxidation (slow; converts bilirubin to polar oxidation products). LED phototherapy delivers higher irradiance (over 30 microwatts/cm2/nm) than older fluorescent lamps. Complications — hyperthermia, dehydration, loose stools, retinal damage (protect with eye shields), separation from mother; and the bronze-baby syndrome in conjugated hyperbilirubinemia (do not phototherapy conjugated jaundice).
Why is early recognition of biliary atresia the surgical emergency of neonatal jaundice?
Biliary atresia is a progressive fibro-obliterative destruction of the extrahepatic biliary tree, presenting with conjugated hyperbilirubinemia (direct fraction over 2 mg/dL or over 20 percent of total), pale acholic stools and dark urine typically after 2 weeks of life. The Kasai portoenterostomy — mobilising a Roux-en-Y jejunal limb up to the porta hepatis after excision of the fibrous biliary remnant — restores bile drainage when done before 60 days (about 80 percent bile drainage), but success falls sharply after 90 days (under 20 percent bile drainage). Every neonate jaundiced beyond 14 days needs a split-bilirubin — an elevated direct fraction mandates urgent HIDA scan, USG (triangular-cord sign), liver biopsy and referral to a paediatric hepatobiliary centre. Kasai failure or late presentation leads to liver transplant.
What is kernicterus and how is it prevented?
Kernicterus (bilirubin-induced neurologic dysfunction, BIND) is the neurological syndrome caused by unconjugated bilirubin crossing the blood-brain barrier and staining the basal ganglia (especially the globus pallidus), hippocampus and subthalamic nuclei. Acute phase — lethargy, poor feeding, hypotonia progressing to hypertonia, opisthotonus, retrocollis, high-pitched cry and seizures. Chronic phase — choreoathetoid cerebral palsy, upgaze palsy (setting-sun sign), sensorineural hearing loss and enamel dysplasia. Prevention centres on pre-discharge Bhutani screening of every newborn, timely phototherapy (LED at 30 microwatts/cm2/nm) at threshold, exchange transfusion (double-volume with cross-matched irradiated blood) for TSB above the exchange line or when bilirubin-to-albumin (B/A) ratio exceeds 8, and G6PD screening (national programme) in high-prevalence populations.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: July 2026