Acute Leukemias MCQ — NEET PG Practice Question | NEETPGAI
Acute Leukemias
medium
microscope Pathology
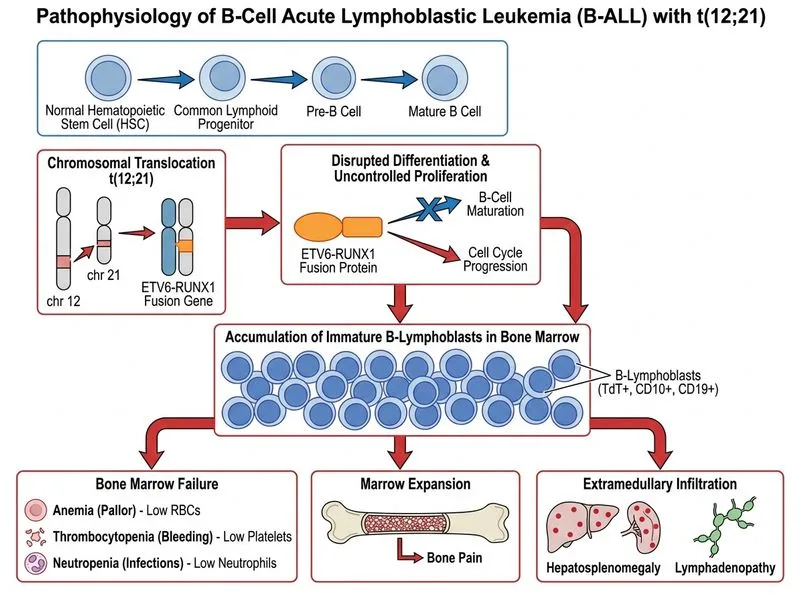
A 6-year-old boy from Mumbai presents with a 2-month history of progressive pallor, bone pain, and recurrent infections. On examination, he has hepatosplenomegaly and generalized lymphadenopathy. Complete blood count shows: Hb 6.8 g/dL, WBC 8,500/μL (65% blasts), platelets 45,000/μL. Bone marrow examination reveals >90% blasts that are TdT+, CD10+, CD19+, CD20−, cIg−. Cytogenetics shows t(12;21)(p13;q22). What is the most likely diagnosis?
A. Lymphoblastic lymphoma with secondary leukemia
B. T-cell acute lymphoblastic leukemia (T-ALL)
C. B-cell acute lymphoblastic leukemia (B-ALL) with t(12;21) — ETV6-RUNX1 fusion
Blasts 65% in peripheral blood — diagnostic for leukemia
Immunophenotype & Morphology
Table
Feature
B-ALL (Common)
T-ALL
Burkitt
This Case
TdT
+
+
−
+ ✓
CD10
+ (common ALL)
−
−
+ ✓
CD19
+ (B-lineage)
−
+
+ ✓
CD20
− or weak
−
+ (strong)
− ✓
cIg
− (immature)
−
+ (surface Ig)
− ✓
Cytogenetics
t(12;21) is favorable
t(9;22), t(1;19)
t(8;14)
t(12;21) ✓
Key Point
The CD10+ CD19+ CD20− cIg− TdT+ immunophenotype defines common B-ALL (cALL), which accounts for ~80% of childhood ALL. This is the most favorable ALL subtype in children.
Cytogenetic Significance: t(12;21) — ETV6-RUNX1
High-YieldNEET PG
The t(12;21)(p13;q22) translocation results in the ETV6-RUNX1 fusion gene and is:
Present in 20–25% of childhood B-ALL — the most common translocation in pediatric ALL
Associated with excellent prognosis — >90% 5-year event-free survival with modern chemotherapy
Detectable by RT-PCR — more sensitive than conventional cytogenetics
NOT associated with t(9;22) (Philadelphia chromosome) — which has poor prognosis
Clinical Pearl
ETV6-RUNX1 fusion is a favorable risk factor that allows for reduced-intensity chemotherapy in some protocols, whereas t(9;22) (BCR-ABL) requires tyrosine kinase inhibitors (imatinib) + intensive chemotherapy.