A 6-year-old boy from rural India presents with 3 weeks of fever, bone pain, and hepatosplenomegaly. CBC shows Hb 8.5 g/dL, WBC 120,000/µL with 70% blasts, platelets 45,000/µL. Flow cytometry confirms B-cell ALL. Uric acid is 9.2 mg/dL, creatinine 1.8 mg/dL (age-adjusted upper limit 0.8), LDH 2400 U/L. What is the most appropriate immediate management before starting chemotherapy?
A. Give rasburicase 0.2 mg/kg IV, hydrate, and monitor; start chemotherapy once uric acid <7 mg/dL and creatinine improves
B. Start allopurinol 10 mg/kg/day and begin induction chemotherapy within 24 hours
C. Initiate IV hydration (3 L/m²/day), allopurinol, and monitor uric acid and creatinine; start chemotherapy only after uric acid normalizes
D. Perform urgent hemodialysis, then start chemotherapy immediately
Explanation
Clinical Context
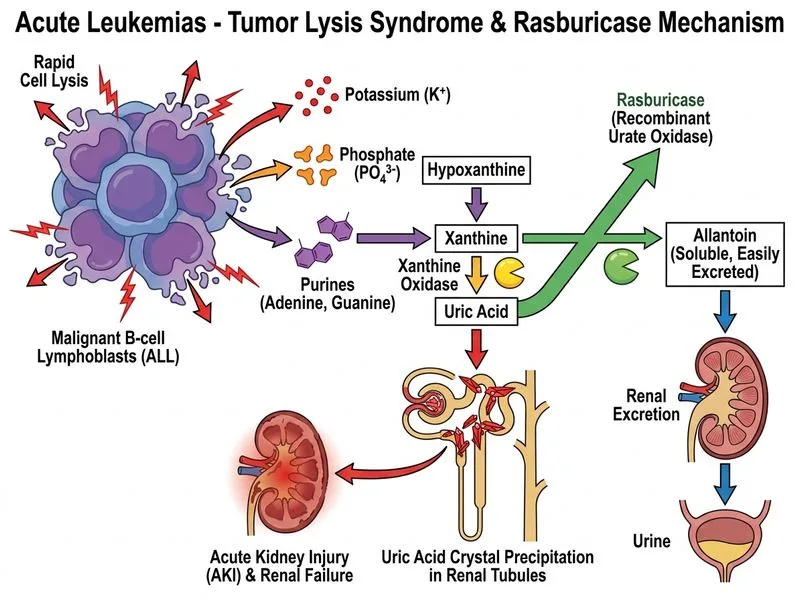
This child has high-risk B-ALL with tumor lysis syndrome (TLS) risk — evidenced by:
Xanthine oxidase inhibitor; reduces uric acid production
Onset
Rapid (within 30 min–4 hrs)
Slow (24–48 hrs)
Efficacy in TLS
Superior; reduces uric acid by 90%
Moderate; takes days to be effective
Renal dysfunction
Safe; works even in AKI
Contraindicated in severe renal failure (risk of xanthine precipitation)
Cost
Higher
Lower
Use in India
Available in tertiary centers
Widely used but slower
Key Point
Allopurinol is contraindicated or ineffective in acute kidney injury because it cannot prevent the acute surge of uric acid from tumor lysis, and it increases xanthine levels (which can precipitate in renal tubules).
Correct Management Sequence
1.
Rasburicase 0.2 mg/kg IV — rapidly converts existing uric acid to allantoin
2.
Aggressive IV hydration — promotes urine output and flushes uric acid
Start chemotherapy only after uric acid normalizes (<7 mg/dL) and creatinine begins to improve
Clinical Pearl
In India, rasburicase availability may be limited in rural centers. If unavailable, allopurinol + hydration + frequent monitoring is the alternative, but rasburicase is the gold standard.
Why Immediate Chemotherapy Is Dangerous
Starting chemotherapy before controlling uric acid will cause: