## Diagnosis: Acute Myelomonocytic Leukemia (AML-M4) ### Key Clinical Features **Key Point:** The combination of Auer rods, positive MPO/SBB stains, CD33+/CD13+ myeloid markers, and HLA-DR+ expression with hepatosplenomegaly and lymphadenopathy is diagnostic of AML-M4 (FAB classification). ### Diagnostic Criteria for AML-M4 | Feature | Finding | Significance | |---------|---------|---------------| | **Morphology** | Medium-sized blasts, abundant cytoplasm, prominent nucleoli | Myelomonocytic differentiation | | **Cytochemistry** | MPO+, SBB+ | Myeloid lineage commitment | | **Immunophenotype** | CD33+, CD13+, HLA-DR+ | Immature myeloid cells | | **Cytogenetics** | Often t(9;11) or other KMT2A rearrangements | Prognostic significance | | **Auer Rods** | Present in some blasts | Indicates myeloid differentiation | ### Pathophysiology 1. **Blast Morphology:** Medium-sized cells with abundant cytoplasm and prominent nucleoli indicate myelomonocytic differentiation (not pure monocytic as in M5). 2. **Cytochemical Profile:** Positive MPO and SBB confirm myeloid lineage; this rules out pure monocytic leukemia (M5). 3. **Immunophenotype:** CD33 and CD13 are myeloid-associated antigens; HLA-DR positivity indicates immature phenotype. 4. **Auer Rods:** Pathognomonic for acute myeloid leukemias; their presence confirms AML rather than ALL. ### High-Yield Differentiating Points **High-Yield:** AML-M4 typically presents with: - Moderate WBC elevation (often 20,000–100,000/μL) - Hepatosplenomegaly and lymphadenopathy (monocytic component) - Auer rods (myeloid component) - Positive MPO/SBB (myeloid differentiation) - CD33+, CD13+, HLA-DR+ (immature myeloid) ### Why This Is Not APL (M3) **Clinical Pearl:** APL (M3) classically presents with: - Abnormal promyelocytes with heavy granulation and multiple Auer rods ("faggot cells") - Severe coagulopathy and DIC (not mentioned here) - t(15;17) translocation (PML-RARA fusion) - Excellent prognosis with ATRA + arsenic trioxide - The blasts here are described as "medium-sized" with "abundant cytoplasm," not the characteristic abnormal promyelocytes of M3. ### Treatment Implications **Key Point:** AML-M4 is treated with intensive chemotherapy (7+3 regimen: cytarabine + daunorubicin/idarubicin), followed by consolidation and possible allogeneic stem cell transplantation depending on cytogenetics and response. ### FAB Classification Context **Mnemonic:** FAB-AML subtypes = **M0–M7** - M0: Undifferentiated AML - M1: AML with minimal differentiation - M2: AML with differentiation (t(8;21)) - **M4: Acute myelomonocytic leukemia** ← This case - M5: Acute monocytic/monocytic leukemia - M6: Acute erythroid leukemia - M7: Acute megakaryoblastic leukemia [cite:Robbins 10e Ch 13] 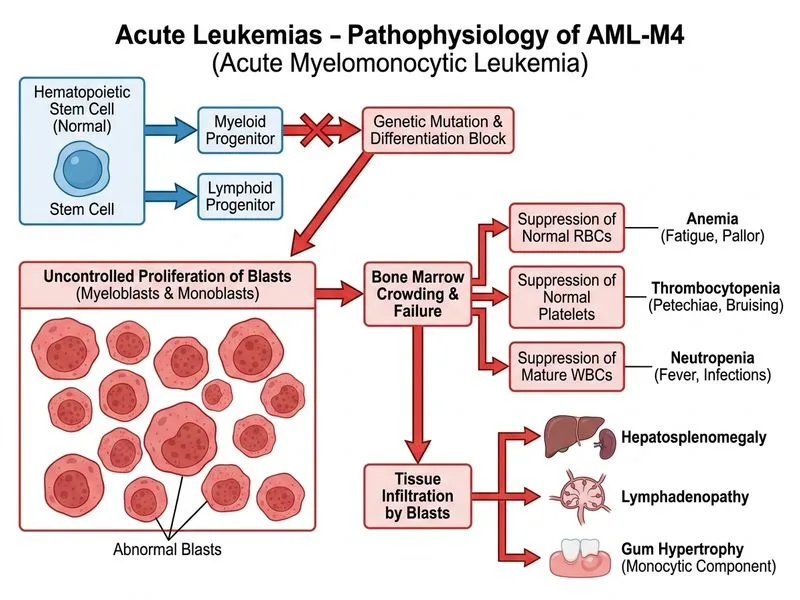
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.