## Prognostically Favorable Translocations in Acute Leukemias **Key Point:** t(15;17) PML-RARA is the defining cytogenetic abnormality of acute promyelocytic leukemia (APL/AML-M3) and carries the **best prognosis** among all acute myeloid leukemias when treated with ATRA and arsenic trioxide. ### t(15;17) PML-RARA in APL **High-Yield:** This translocation results in fusion of the **promyelocytic leukemia (PML) gene** on chromosome 15 with the **retinoic acid receptor alpha (RARA) gene** on chromosome 17. #### Mechanism of ATRA Sensitivity 1. The PML-RARA fusion protein acts as an aberrant transcriptional repressor 2. ATRA binds to the RARA domain and causes: - Degradation of the fusion protein - Release of transcriptional repression - Differentiation of leukemic promyelocytes into mature neutrophils - Restoration of normal apoptosis **Clinical Pearl:** APL with t(15;17) has transformed from a **fatal disease** (historically 80% mortality from DIC) to a **highly curable disease** (>90% cure rate) with ATRA + arsenic trioxide combination therapy. ### Comparison of Translocations in Acute Leukemias | Translocation | Leukemia Type | Prognosis | Targeted Therapy | Cure Rate | | --- | --- | --- | --- | --- | | **t(15;17)** | **APL (AML-M3)** | **Excellent** | **ATRA + ATO** | **>90%** | | t(9;22) | CML/B-ALL | Poor (CML) | Tyrosine kinase inhibitors | Variable | | t(8;14) | Burkitt lymphoma/ALL | Poor | Chemotherapy | 50–90% (pediatric) | | t(4;11) | Infant ALL/AML | Very poor | Chemotherapy | <40% | **Mnemonic:** **"APL-15-17 = ATRA-Responsive Transformation"** — t(15;17) is the only acute leukemia translocation with a specific, highly effective targeted therapy that induces differentiation rather than just cytotoxicity. **Warning:** Do not confuse t(15;17) with other translocations in AML — only t(15;17) defines APL and confers ATRA sensitivity. Other AML translocations (e.g., t(8;21), t(15;17) inv(16)) have different prognoses and do not respond to ATRA. 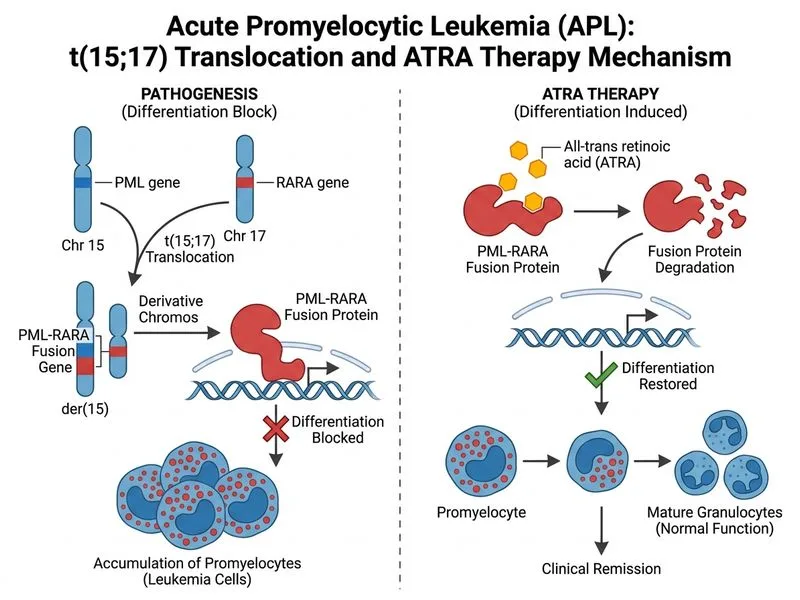
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.