## Clinical Diagnosis: Primary Adrenal Insufficiency ### Key Diagnostic Features **Key Point:** The combination of low cortisol with **elevated ACTH** is pathognomonic for primary adrenal insufficiency (Addison disease). The adrenal gland is damaged, so it cannot produce cortisol despite maximal pituitary stimulation. ### Laboratory Interpretation | Parameter | Patient Value | Normal Range | Interpretation | |-----------|---------------|--------------|----------------| | Morning cortisol | 2.2 µg/dL | >10 µg/dL | Severely low | | ACTH | 285 pg/mL | <46 pg/mL | Markedly elevated | | Na⁺ | 128 mEq/L | 135–145 mEq/L | Hyponatremia | | K⁺ | 5.8 mEq/L | 3.5–5.0 mEq/L | Hyperkalemia | **High-Yield:** The **low cortisol + high ACTH** pattern is the gold standard for diagnosing primary adrenal insufficiency. In secondary insufficiency (pituitary disease), ACTH would be low or inappropriately normal. ### Clinical Presentation Correlation 1. **Hyperpigmentation** — due to elevated ACTH stimulating melanocytes (ACTH is derived from pro-opiomelanocortin) 2. **Hyponatremia & hyperkalemia** — loss of aldosterone secretion (zona glomerulosa atrophy) 3. **Hypotension** — combined loss of cortisol and aldosterone 4. **Hypoglycemia** — loss of cortisol's gluconeogenic effect 5. **Weakness & weight loss** — chronic cortisol deficiency **Clinical Pearl:** Hyperpigmentation in the setting of hyponatremia and hypotension is a clinical red flag for Addison disease. This triad is rarely seen in secondary adrenal insufficiency. ### Pathophysiology Diagram ```mermaid flowchart TD A[Adrenal cortex destruction<br/>Autoimmune/TB/Infiltration]:::urgent --> B[Loss of cortisol production] A --> C[Loss of aldosterone production] B --> D[Hypoglycemia<br/>Weakness<br/>Hypotension]:::outcome C --> E[Hyponatremia<br/>Hyperkalemia<br/>Hypotension]:::outcome B --> F[Pituitary responds with<br/>increased ACTH release]:::action F --> G[ACTH stimulates melanocytes]:::action G --> H[Hyperpigmentation]:::outcome ``` **Mnemonic:** **ACTH-HIGH in Primary, ACTH-LOW in Secondary** — Remember: in primary disease, the pituitary tries hard (high ACTH); in secondary disease, the pituitary is broken (low ACTH). ### Confirmatory Tests - **Short Synacthen (ACTH stimulation) test:** Cortisol fails to rise >18 µg/dL after 250 µg IV ACTH in primary insufficiency - **Imaging:** Adrenal CT/MRI to identify autoimmune atrophy, tuberculosis, or infiltration - **Autoantibodies:** 21-hydroxylase antibodies (most common in autoimmune Addison disease) [cite:Harrison 21e Ch 375] 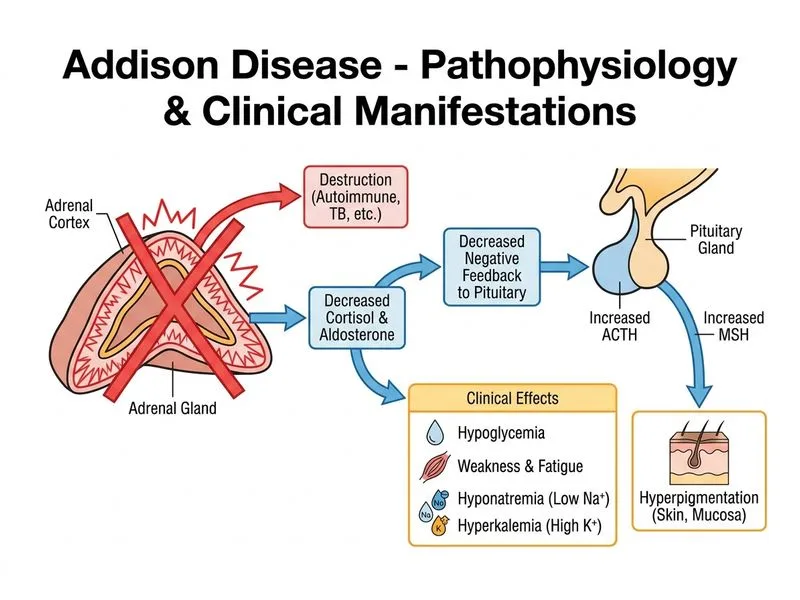
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.