## Management of Acute Adrenal Crisis ### Clinical Context: Addisonian Crisis **Key Point:** This patient is in **acute adrenal crisis** — a life-threatening emergency characterized by severe hypotension, hyponatremia, hypoglycemia, and altered mental status. The underlying cause is likely tuberculous destruction of the adrenal glands (Addison disease). **High-Yield:** In acute adrenal crisis, **high-dose hydrocortisone IV is the immediate, life-saving intervention**. It must be given before or simultaneously with diagnostic confirmation. ### Why Hydrocortisone is Correct | Feature | Hydrocortisone | Dexamethasone | Fludrocortisone | Prednisone | |---------|----------------|---------------|-----------------|------------| | **Route in crisis** | IV (rapid onset) | IV (but not first-line) | Oral (too slow) | Oral (too slow) | | **Glucocorticoid potency** | 1× (physiologic) | 25–30× (excessive) | Minimal | 4× | | **Mineralocorticoid activity** | Moderate (helpful) | None | Very high | Minimal | | **Onset of action** | Minutes (IV) | Minutes (IV) | Hours (oral) | Hours (oral) | | **Dosing in crisis** | 100 mg stat, then 50–100 mg q6–8h | Not recommended in crisis | Not first-line | Not appropriate | **Clinical Pearl:** Hydrocortisone is the **only glucocorticoid with inherent mineralocorticoid activity**. This is crucial in acute crisis when both cortisol and aldosterone are deficient. ### Pathophysiology of Adrenal Crisis ```mermaid flowchart TD A[Severe adrenal insufficiency<br/>TB, autoimmune, or infiltration]:::urgent --> B[Acute stressor<br/>Infection, trauma, surgery] B --> C[Cortisol cannot increase<br/>Aldosterone depleted]:::urgent C --> D[Severe hypotension<br/>Hypovolemia<br/>Shock]:::urgent C --> E[Hyponatremia<br/>Hyperkalemia<br/>Hypoglycemia]:::urgent D --> F[Altered mental status<br/>Cardiovascular collapse]:::urgent F --> G[IV Hydrocortisone 100 mg stat]:::action G --> H[Rapid restoration of<br/>cortisol & aldosterone effect]:::action H --> I[BP stabilizes<br/>Electrolytes improve<br/>Survival]:::outcome ``` ### Treatment Protocol for Adrenal Crisis **Immediate (First 24 hours):** 1. **Hydrocortisone 100 mg IV stat** 2. **Then 50–100 mg IV every 6–8 hours** (or continuous infusion 200–300 mg/day) 3. **Aggressive IV fluid resuscitation** with normal saline (0.9% NaCl) — addresses hypovolemia and hyponatremia 4. **Treat underlying precipitant** (antibiotics for infection, as in this case) **Transition (After 24–48 hours, as crisis resolves):** - Reduce hydrocortisone to 50 mg every 6 hours - Then transition to oral replacement (typically 15–20 mg cortisol equivalent daily) - Add **fludrocortisone 0.1 mg oral daily** for mineralocorticoid replacement (once acute phase is over) **Mnemonic:** **HI-DOSE hydrocortisone in CRISIS** — High-dose, IV, Dexamethasone is not first-line, Ongoing fluids, Steroids early, Electrolyte monitoring, Underlying cause treated. ### Why Other Options Are Wrong **Dexamethasone (Option 2):** - Dexamethasone is 25–30× more potent than hydrocortisone - It has **no mineralocorticoid activity** — critical deficiency in acute crisis - It is reserved for diagnostic ACTH suppression testing or chronic replacement when hydrocortisone is unavailable - In acute crisis, the excessive potency and lack of mineralocorticoid effect make it inferior to hydrocortisone **Fludrocortisone (Option 3):** - Fludrocortisone is a **mineralocorticoid with weak glucocorticoid activity** - It is **not sufficient** for acute crisis, which requires rapid, high-dose glucocorticoid replacement - It is used as **adjunctive therapy** in chronic Addison disease (0.05–0.1 mg daily), not as monotherapy in crisis - Oral route is too slow for a hemodynamically unstable patient **Prednisone (Option 4):** - Oral route is inappropriate in acute crisis with altered mental status and shock - Prednisone has 4× glucocorticoid potency but no mineralocorticoid activity - Onset is too slow (1–2 hours) compared to IV hydrocortisone (minutes) [cite:Harrison 21e Ch 375; Endocrine Society Clinical Practice Guidelines for Adrenal Insufficiency] 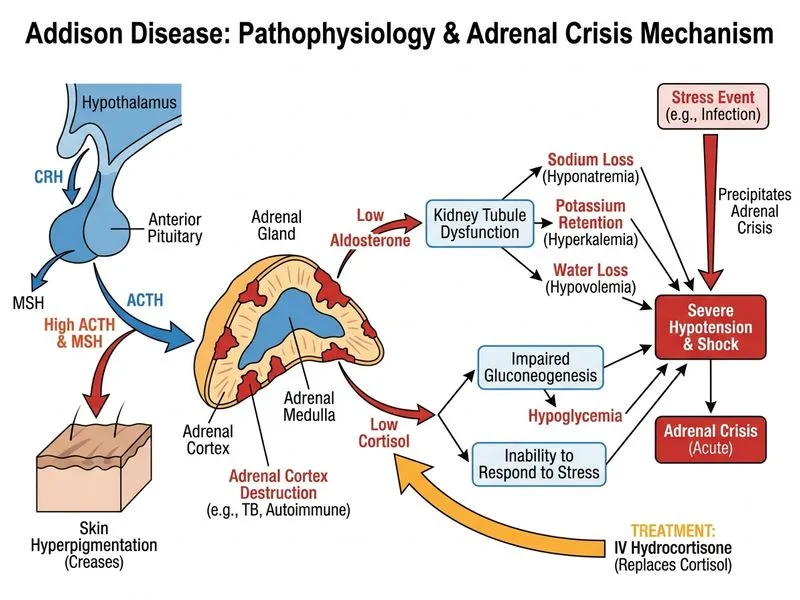
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.