## Clinical Diagnosis: Primary Adrenal Insufficiency (Addison Disease) ### Key Clinical Features Present **Key Point:** The constellation of hyperpigmentation + hyponatremia + hyperkalemia + hypoglycemia + hypotension + low morning cortisol is pathognomonic for primary adrenal insufficiency. ### Pathophysiology 1. **Cortisol deficiency** → hypoglycemia, hypotension, weakness, syncope 2. **Aldosterone deficiency** → sodium loss, potassium retention, volume depletion 3. **Loss of negative feedback on ACTH** → ACTH rises markedly 4. **ACTH stimulates melanocytes** → hyperpigmentation of skin and mucosa (especially buccal mucosa, creases, areolae) ### Diagnostic Criteria Met | Feature | Finding | Significance | |---------|---------|---------------| | **Hyperpigmentation** | Diffuse skin + oral mucosa | ACTH-driven (primary insufficiency only) | | **Hyponatremia** | 128 mEq/L | Aldosterone loss + SIADH from stress | | **Hyperkalemia** | 6.2 mEq/L | Aldosterone deficiency | | **Hypoglycemia** | 62 mg/dL | Cortisol deficiency | | **Low cortisol** | 3.2 µg/dL (morning) | Confirms adrenal failure | | **Hypotension** | 92/58 mmHg | Cortisol + aldosterone loss | ### Why This Is Primary, Not Secondary **High-Yield:** Secondary adrenal insufficiency (pituitary/hypothalamic) presents with **low cortisol BUT normal or low ACTH**, and **NO hyperpigmentation** (ACTH is suppressed). In this case, the clinical hyperpigmentation strongly indicates elevated ACTH, which only occurs in primary adrenal failure. ### Confirmatory Tests 1. **ACTH level** — will be markedly elevated (>100 pg/mL) in primary insufficiency 2. **Aldosterone level** — low, with elevated plasma renin activity 3. **Etiology workup** — TB serology, adrenal imaging (CT/MRI), autoimmune markers (21-hydroxylase antibodies) — TB is the leading cause in India **Clinical Pearl:** In India, tuberculosis is the most common cause of Addison disease (40–50% of cases), followed by autoimmune adrenalitis. Always screen for TB in any suspected case. ### Immediate Management 1. **IV hydrocortisone 100 mg stat, then 50–100 mg every 6–8 hours** (adrenal crisis) 2. **Normal saline 500 mL bolus** for hypovolemia and hyponatremia 3. **Dextrose 5–10% IV** for hypoglycemia 4. **Monitor K⁺, Na⁺, glucose** closely 5. **Once stabilized:** long-term glucocorticoid + mineralocorticoid replacement **Mnemonic: ADDISON** — **A**drenal insufficiency, **D**ark skin, **D**ehydration, **I**ncreased ACTH, **S**odium loss, **O**rthostatism, **N**eed steroids 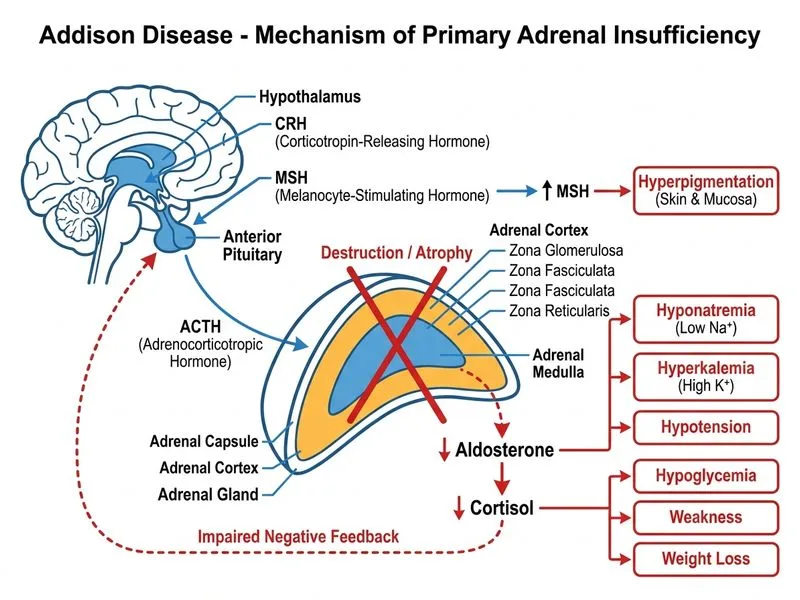
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.