## Acute Adrenal Crisis: Emergency Management ### Clinical Context: Acute Addisonian Crisis This patient presents with **adrenal crisis** — a life-threatening emergency characterized by acute decompensation of adrenal function. The clinical and biochemical picture is unambiguous: | Finding | Interpretation | |---------|----------------| | **Severe hypotension** (78/50) | Acute cortisol + aldosterone loss | | **Severe hyponatremia** (118) | Aldosterone deficiency + SIADH | | **Severe hyperkalemia** (6.8) | Aldosterone deficiency | | **Severe hypoglycemia** (48) | Cortisol deficiency | | **Confusion + weakness** | Hypoglycemia + electrolyte derangement | | **Low cortisol + very high ACTH** | Primary adrenal failure | | **Hyperpigmentation** | Elevated ACTH (primary insufficiency) | | **TB history** | TB-induced adrenalitis (most likely etiology) | ### Why This Is a Medical Emergency **Key Point:** Adrenal crisis is a medical emergency with mortality >5% if untreated. The patient is in shock with life-threatening electrolyte abnormalities and severe hypoglycemia. **Immediate treatment is required — do not delay for confirmatory tests.** ### Correct Management: Immediate Intervention **High-Yield:** In suspected adrenal crisis, **treat first, confirm later**. Do NOT wait for test results. 1. **IV Hydrocortisone 100 mg stat** (bolus) 2. **Followed by 50–100 mg every 6–8 hours** (or continuous infusion 10 mg/hour) 3. **IV Normal Saline 500 mL bolus** (or more, depending on response) 4. **Dextrose 5–10% IV** for hypoglycemia 5. **Monitor vital signs, K⁺, Na⁺, glucose** closely 6. **Once stabilized (24–48 hours):** transition to oral glucocorticoid + mineralocorticoid replacement ### Why Hydrocortisone? - **Hydrocortisone** (cortisol) has both glucocorticoid AND mineralocorticoid activity - **Dexamethasone** or **prednisolone** lack mineralocorticoid activity and are inappropriate in acute crisis - **Dosing:** 100 mg IV is the standard acute dose; this is 20× the usual daily replacement dose ### Pathophysiology of Crisis ```mermaid flowchart TD A[TB-induced adrenalitis]:::outcome --> B[Destruction of adrenal cortex] B --> C[Acute loss of cortisol + aldosterone] C --> D[Hypotension + shock]:::urgent C --> E[Hyponatremia + hyperkalemia]:::urgent C --> F[Hypoglycemia]:::urgent D --> G[Altered mental status] E --> H[Cardiac arrhythmias] F --> I[Seizures] G --> J[Death if untreated]:::urgent K[IV Hydrocortisone 100 mg]:::action --> L[Reverses shock] K --> M[Corrects electrolytes] K --> N[Corrects hypoglycemia] ``` **Clinical Pearl:** TB destroys the adrenal cortex gradually, but an acute stressor (infection, surgery, medication non-compliance) can precipitate sudden decompensation. This patient likely missed doses of anti-TB drugs or developed a superimposed infection. ### Why the Other Options Are Wrong **Tip:** In an acute crisis, diagnostic confirmation tests are a **trap**. The patient is in shock and needs immediate treatment. 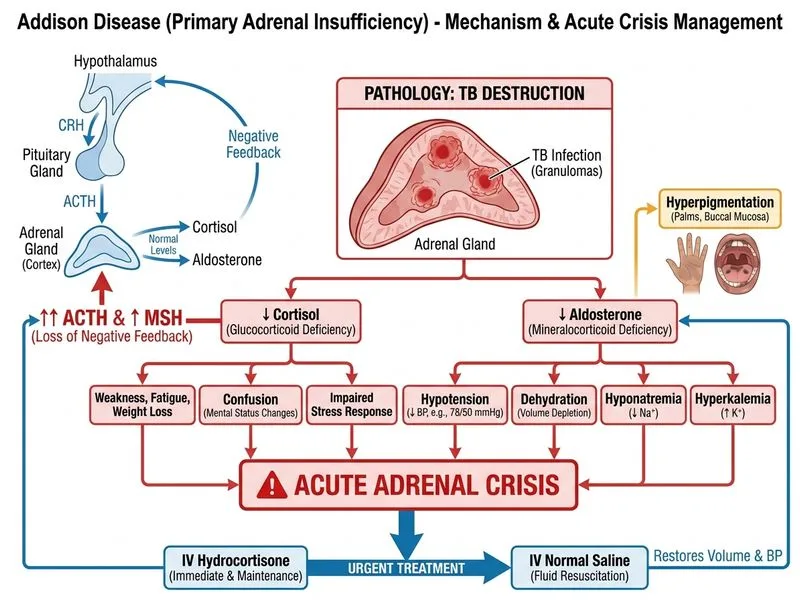
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.