## Adynamic Bone Disease in CKD-MBD **Key Point:** Adynamic bone disease (ABD) is characterized by **low bone turnover with minimal osteoid** and is increasingly common in dialysis patients. It is distinct from high-turnover disease (osteitis fibrosa) and requires careful management to avoid worsening. ### Pathophysiology: 1. **Etiology:** Over-suppression of PTH (from excessive vitamin D, calcium, or calcimimetics), aluminum accumulation, or uremia-induced osteoblast dysfunction. 2. **Histology:** Low bone formation rate, minimal osteoid, reduced osteoblast activity — the **hallmark** of ABD. 3. **Clinical presentation:** Bone pain, muscle weakness, fractures; paradoxically, PTH may be elevated (secondary HPT) but bone turnover is suppressed. 4. **Biochemistry:** Elevated PTH with low-normal or normal alkaline phosphatase (as seen here: ALP 120, PTH 850). ### Management of ABD: - **Avoid aggressive PTH suppression:** Do NOT use cinacalcet or high-dose vitamin D analogs (these worsen ABD). - **Vitamin D analogs** (calcitriol, paricalcitol) at **low-to-moderate doses** to stimulate bone turnover. - **Increase dialysate calcium** (from 2.5 to 3.0 mEq/L) to provide positive calcium balance and stimulate osteoblasts. - **Reduce calcium-based phosphate binders** to avoid hypercalcemia. - **Monitor PTH:** Target 150–300 pg/mL in dialysis patients (higher than in non-dialysis CKD) to maintain bone turnover. **Clinical Pearl:** ABD is a **low-turnover disease** requiring stimulation, NOT suppression. Cinacalcet and aggressive vitamin D would worsen outcomes. **High-Yield:** The combination of **elevated PTH + low ALP + low osteoid** is pathognomonic for ABD. Management is the opposite of osteitis fibrosa (high-turnover disease). 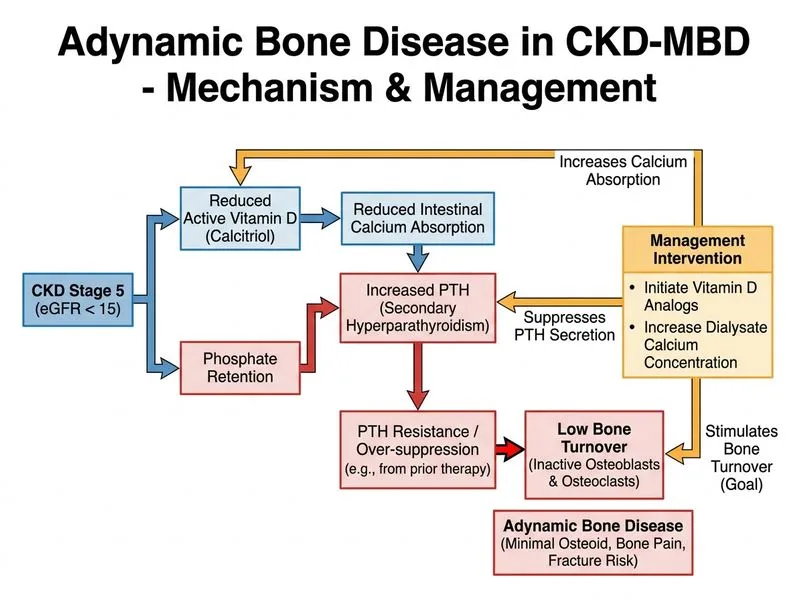
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.