## Anemia Management in CKD Stage 4–5 **Key Point:** ESA initiation in CKD-related anemia requires iron sufficiency assessment and a hemoglobin threshold of <10 g/dL (or 10–11 g/dL if symptomatic), per KDIGO 2021 guidelines. ### Rationale: - **Iron assessment is mandatory** before ESA use. Functional iron deficiency is common in CKD; ESAs are ineffective without adequate iron stores (ferritin ≥100 ng/mL, TSAT ≥20%). - **Hemoglobin target:** Current evidence-based practice avoids targeting Hb >11 g/dL in CKD, as higher targets increase thrombotic and cardiovascular risk without mortality benefit. - **This patient's Hb 8.5 g/dL** warrants investigation of iron status before ESA initiation; if iron-replete, ESA is appropriate at Hb <10 g/dL. - Iron supplementation alone is insufficient if iron stores are adequate; ESA is needed for EPO-responsive anemia. **Clinical Pearl:** Normocytic anemia in CKD is primarily EPO-responsive; however, iron deficiency (absolute or functional) is a common co-factor limiting ESA efficacy. **High-Yield:** KDIGO recommends checking iron indices (ferritin, TSAT) before and during ESA therapy; target TSAT 20–50% and ferritin 100–500 ng/mL. 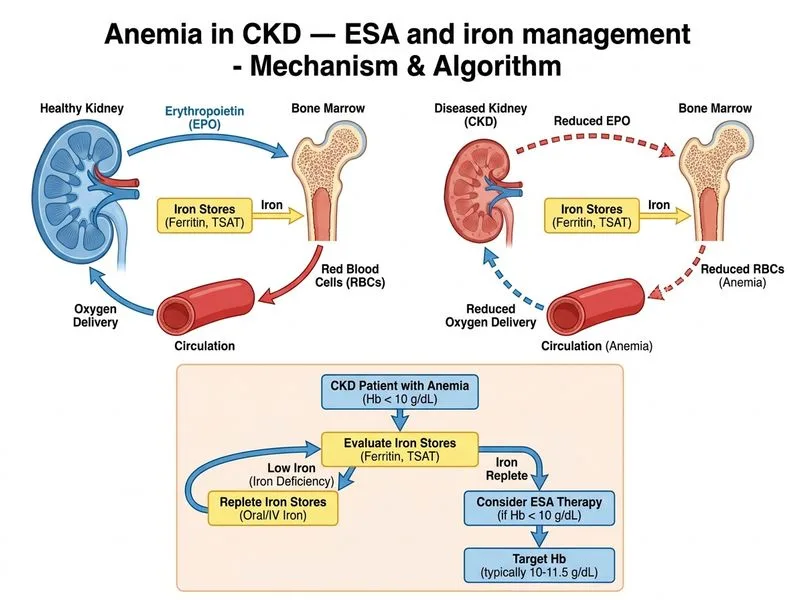
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.