## Clinical Reasoning This patient presents with a constellation of findings highly suggestive of **thalassemia major**: ### Key Diagnostic Features **Key Point:** The combination of severe microcytic anemia (MCV 58 fL), elevated reticulocyte count (8%), and indirect hyperbilirubinemia indicates both chronic hemolysis and ineffective erythropoiesis. **High-Yield:** Thalassemia major classically presents with: - Microcytic hypochromic anemia (often MCV <60 fL) - Target cells on blood smear (pathognomonic finding) - Marked reticulocytosis (compensatory response to hemolysis) - Indirect hyperbilirubinemia (from RBC destruction) - Secondary iron overload (from repeated transfusions and increased intestinal absorption) ### Iron Metabolism Pattern | Parameter | Thalassemia Major | Iron Deficiency | Sideroblastic | |-----------|------------------|-----------------|----------------| | Serum Iron | ↑ (high) | ↓ (low) | ↑ (high) | | Ferritin | ↑ (high) | ↓ (low) | ↑ (high) | | TIBC | Normal/↓ | ↑ (high) | Normal/↓ | | Reticulocyte Count | ↑↑ (8–10%) | ↓ (low) | Variable | | Bilirubin (indirect) | ↑ | Normal | Normal/↑ | **Clinical Pearl:** The elevated serum iron and ferritin with *normal* TIBC (not elevated) rules out iron deficiency. The high reticulocyte count and indirect hyperbilirubinemia confirm hemolysis, not just microcytic production. ### Pathophysiology in This Case In thalassemia major, defective β-globin chain synthesis leads to: 1. Imbalanced globin chains → precipitation of excess α-chains 2. Ineffective erythropoiesis (destruction of erythroblasts in marrow) 3. Chronic hemolysis of surviving RBCs 4. Compensatory erythroid hyperplasia → increased iron absorption 5. Transfusion-dependent anemia → transfusional iron overload **Mnemonic:** THALASSEMIA = **T**arget cells, **H**emolysis (high reticulocytes), **A**nemia (severe, early onset), **L**ow MCV, **A**bsorbed iron (secondary), **S**econdary hemochromatosis, **S**evere, **E**rythroid hyperplasia, **M**icrocytic, **I**neffective erythropoiesis, **A**bnormal Hb pattern ### Why This Presentation Fits Thalassemia Major - **Age of presentation:** Typically manifests in childhood/early adulthood; this patient likely had undiagnosed disease - **Rural setting:** Higher prevalence in endemic areas (Mediterranean, Middle East, South Asia) - **Target cells:** Virtually diagnostic of thalassemia (also seen in liver disease, but clinical context rules this out) - **Indirect hyperbilirubinemia:** Confirms hemolysis - **Elevated reticulocyte count:** Appropriate marrow response to hemolysis - **Secondary iron overload:** Expected finding in transfusion-dependent thalassemia **High-Yield:** Diagnosis is confirmed by hemoglobin electrophoresis showing elevated HbF and HbA2 (>3.5%), with absent or severely reduced HbA. 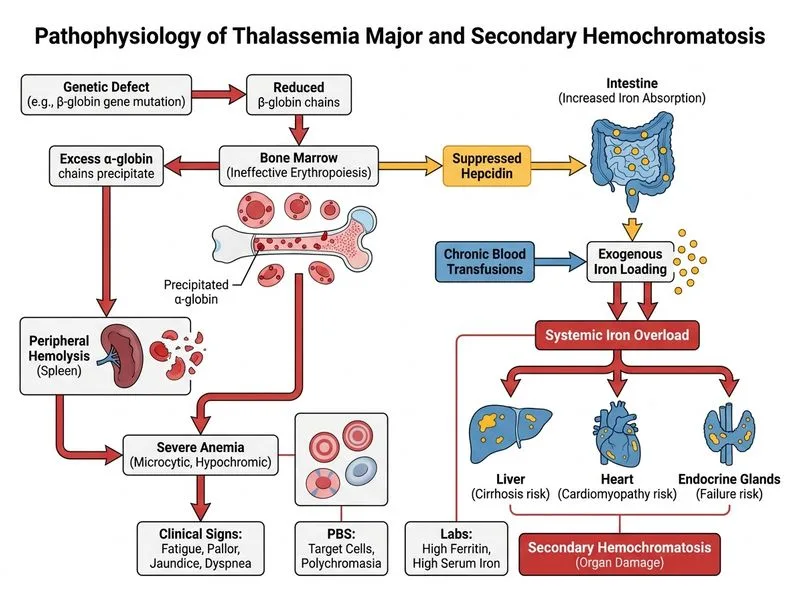
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.