## Clinical Interpretation This patient presents with **macrocytic anemia with pancytopenia and renal dysfunction**, strongly suggestive of **vitamin B12 deficiency** with complications. The next step is to **confirm B12 deficiency at the metabolic level** before pursuing etiology. ### Why Metabolic Confirmation Comes First **Key Point:** A low serum B12 level (180 pg/mL) is necessary but *not sufficient* for diagnosis. Many patients with borderline B12 levels (150–250 pg/mL) are asymptomatic, while others with low-normal levels are truly deficient. Metabolic markers (methylmalonic acid and homocysteine) are the gold standard for confirming functional B12 deficiency. **High-Yield:** In B12 deficiency: - Methylmalonic acid (MMA) is ↑↑ (>0.4 µmol/L) - Homocysteine is ↑↑ (>15 µmol/L) - Both are elevated because B12 is a cofactor for methylmalonyl-CoA mutase and methionine synthase In folate deficiency alone: - MMA is normal (because methylmalonyl-CoA mutase does not require folate) - Homocysteine is elevated (because methionine synthase requires folate) ### Diagnostic Algorithm for Macrocytic Anemia ```mermaid flowchart TD A[Macrocytic Anemia<br/>MCV > 100 fL]:::outcome --> B{Reticulocyte<br/>Count?}:::decision B -->|Low| C[Ineffective Erythropoiesis]:::outcome B -->|Normal/High| D[Hemolysis or Recent<br/>Transfusion]:::outcome C --> E{Check B12<br/>& Folate}:::decision E -->|Both Low| F[Check MMA<br/>& Homocysteine]:::action E -->|B12 Low,<br/>Folate Normal| G[Confirm with MMA<br/>& Homocysteine]:::action E -->|Folate Low,<br/>B12 Normal| H[Folate Deficiency]:::outcome F --> I{MMA ↑?<br/>Hcy ↑?}:::decision I -->|Both ↑| J[B12 Deficiency<br/>Confirmed]:::outcome I -->|Only Hcy ↑| K[Folate Deficiency<br/>or Combined]:::outcome G --> L{MMA ↑?<br/>Hcy ↑?}:::decision L -->|Both ↑| M[B12 Deficiency<br/>Confirmed]:::outcome L -->|Normal| N[Pseudodeficiency or<br/>Other Cause]:::outcome J --> O[Proceed to Etiology:<br/>Intrinsic Factor Abs,<br/>Parietal Cell Abs,<br/>Schilling Test]:::action ``` ### Why Each Step Matters **Clinical Pearl:** The presence of **renal dysfunction** (Cr 2.8 mg/dL) is a critical clue. Homocysteine is renally cleared; elevated homocysteine can cause endothelial injury and acute kidney injury. This bidirectional relationship makes metabolic confirmation urgent. **Mnemonic for B12 Deficiency Complications:** **NEUROPSYCH** = **N**europathy, **E**ncephalopathy, **U**nstable gait, **R**educed reflexes, **O**ptic atrophy, **P**sychosis, **S**ubacute combined degeneration, **Y**ellow-waxy skin, **C**ardiac (high-output), **H**emolytic anemia ### Why Metabolic Markers Are Superior to Serology at This Stage | Investigation | Purpose | Timing | |---|---|---| | **MMA & Homocysteine** | Confirm functional B12 deficiency (metabolic level) | **First** — determines if B12 deficiency is real | | **Intrinsic Factor Antibodies** | Identify pernicious anemia (autoimmune etiology) | Second — only if B12 deficiency confirmed | | **Parietal Cell Antibodies** | Support autoimmune gastritis diagnosis | Second — supportive, not diagnostic | | **Schilling Test** | Determine if malabsorption is due to IF deficiency or ileal disease | Third — rarely done now, replaced by MMA/Hcy | | **Bone Marrow Biopsy** | Assess for dysplasia, malignancy, or other marrow pathology | Only if diagnosis remains unclear | **High-Yield:** The Schilling test is largely obsolete in modern practice because: 1. MMA and homocysteine are more specific and sensitive 2. Schilling test is cumbersome (requires radioactive B12 and 24-hour urine collection) 3. Intrinsic factor antibodies are more practical for confirming pernicious anemia ### Clinical Context in This Patient The combination of: - Macrocytic anemia (MCV 102 fL) - Pancytopenia (WBC 2.1, platelets 35) - Hypersegmented neutrophils (pathognomonic for megaloblastic anemia) - Low-normal B12 (180 pg/mL) - Renal dysfunction ...makes **metabolic confirmation the logical next step**. If MMA and homocysteine are elevated, the diagnosis is B12 deficiency; if normal, consider folate deficiency, hypothyroidism, or other causes of macrocytosis. 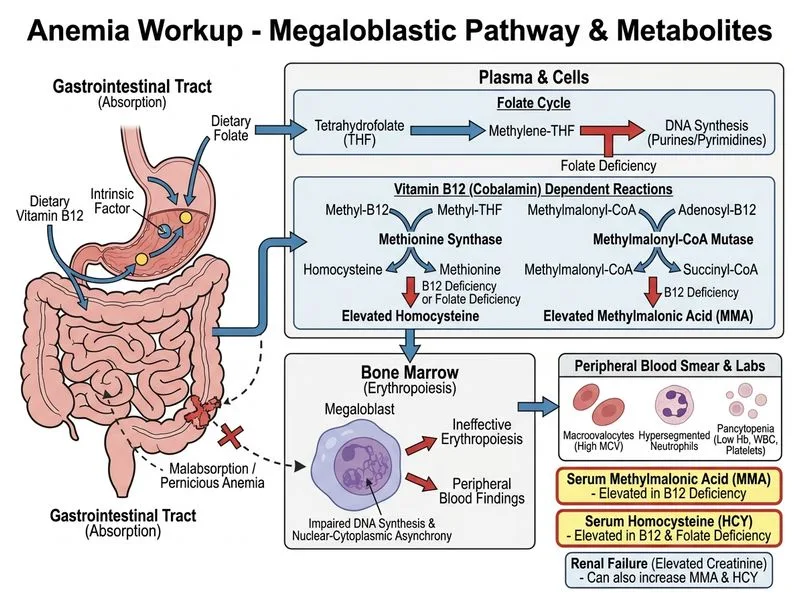
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.